

Effect of surgical experience and spine subspecialty on the reliability of the AO Spine Upper Cervical Injury Classification System
- PMID: 35986731
- PMCID: PMC10193484
- DOI: 10.3171/2022.6.SPINE22454
Effect of surgical experience and spine subspecialty on the reliability of the AO Spine Upper Cervical Injury Classification System
Abstract
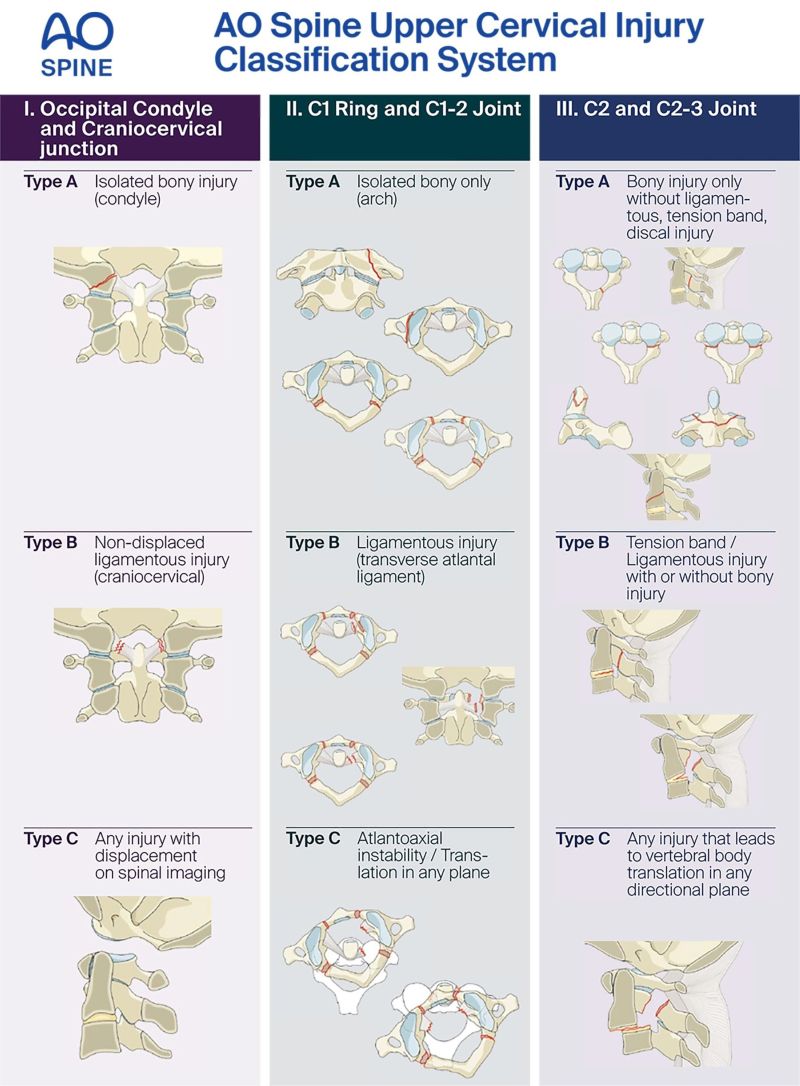
Objective: The objective of this paper was to determine the interobserver reliability and intraobserver reproducibility of the AO Spine Upper Cervical Injury Classification System based on surgeon experience (< 5 years, 5-10 years, 10-20 years, and > 20 years) and surgical subspecialty (orthopedic spine surgery, neurosurgery, and "other" surgery).
Methods: A total of 11,601 assessments of upper cervical spine injuries were evaluated based on the AO Spine Upper Cervical Injury Classification System. Reliability and reproducibility scores were obtained twice, with a 3-week time interval. Descriptive statistics were utilized to examine the percentage of accurately classified injuries, and Pearson's chi-square or Fisher's exact test was used to screen for potentially relevant differences between study participants. Kappa coefficients (κ) determined the interobserver reliability and intraobserver reproducibility.
Results: The intraobserver reproducibility was substantial for surgeon experience level (< 5 years: 0.74 vs 5-10 years: 0.69 vs 10-20 years: 0.69 vs > 20 years: 0.70) and surgical subspecialty (orthopedic spine: 0.71 vs neurosurgery: 0.69 vs other: 0.68). Furthermore, the interobserver reliability was substantial for all surgical experience groups on assessment 1 (< 5 years: 0.67 vs 5-10 years: 0.62 vs 10-20 years: 0.61 vs > 20 years: 0.62), and only surgeons with > 20 years of experience did not have substantial reliability on assessment 2 (< 5 years: 0.62 vs 5-10 years: 0.61 vs 10-20 years: 0.61 vs > 20 years: 0.59). Orthopedic spine surgeons and neurosurgeons had substantial intraobserver reproducibility on both assessment 1 (0.64 vs 0.63) and assessment 2 (0.62 vs 0.63), while other surgeons had moderate reliability on assessment 1 (0.43) and fair reliability on assessment 2 (0.36).
Conclusions: The international reliability and reproducibility scores for the AO Spine Upper Cervical Injury Classification System demonstrated substantial intraobserver reproducibility and interobserver reliability regardless of surgical experience and spine subspecialty. These results support the global application of this classification system.
Keywords: AO Spine; neurosurgeon; orthopedic spine surgeon; reliability; reproducibility; trauma; upper cervical spine.
Conflict of interest statement
The study was funded and supported by AO Spine; statistical support was provided. Dr. Benneker: consultant for Icotec and Kuros; and clinical or research support for the study described (includes equipment or material) from Sentryx. Dr. Bransford: speakers bureau for DePuy Synthes and Globus. Dr. Schnake: consultant for AO Spine International. Dr. Vaccaro: ownership in Advanced Spinal Intellectual Properties, Atlas Spine, Avaz Surgical, AVKN Patient Driven Care, Bonovo Orthopaedics, Computational Biodynamics, Cytonics, Deep Health, Dimension Orthotics LLC, Electrocore, Flagship Surgical, FlowPharma, Globus, Innovative Surgical Design, Jushi, NuVasive, Orthobullets, Parvizi Surgical Innovation, Progressive Spinal Technologies, Replication Medica, Spine Medica, Spineology, Stout Medical, Surgalign, and ViewFi Health; royalties from Aesculap, Atlas Spine, Globus, Medtronic, Spine Wave, and Stryker Spine; and board member of National Spine Health Foundation and Sentryx.
Figures
References
-
- Lowery DW, Wald MM, Browne BJ, Tigges S, Hoffman JR, Mower WR. Epidemiology of cervical spine injury victims. Ann Emerg Med. 2001;38(1):12–16. - PubMed
-
- Jefferson G. Fracture of the atlas vertebra: report of four cases, and a review of those previously recorded. Br J Surg. 1920;7:407–422.
-
- Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine (Phila Pa 1976) 1988;13(7):731–736. - PubMed
-
- Tuli S, Tator CH, Fehlings MG, Mackay M. Occipital condyle fractures. Neurosurgery. 1997;41(2):368–377. - PubMed
