

How to improve intubation in the intensive care unit. Update on knowledge and devices
- PMID: 35986748
- PMCID: PMC9391631
- DOI: 10.1007/s00134-022-06849-0
How to improve intubation in the intensive care unit. Update on knowledge and devices
Abstract
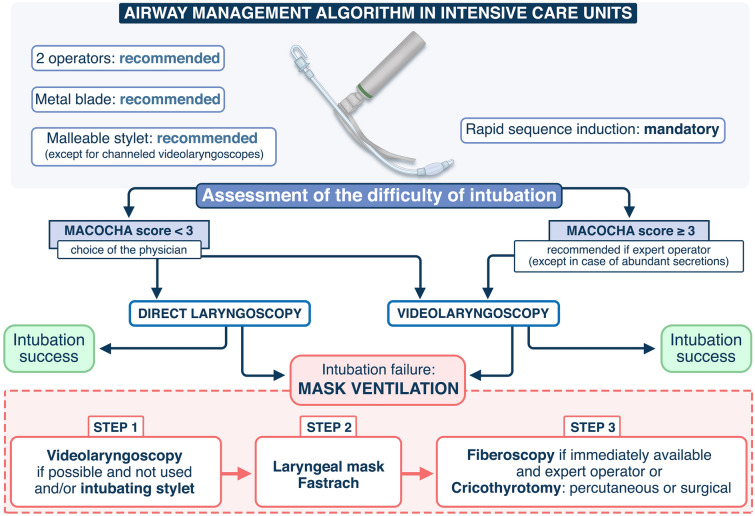
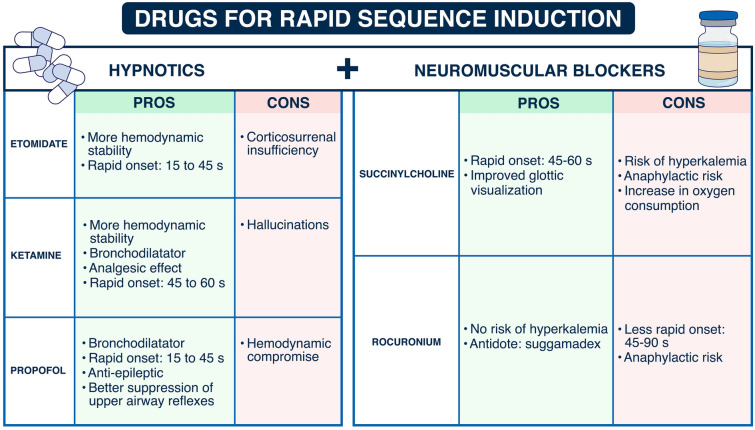
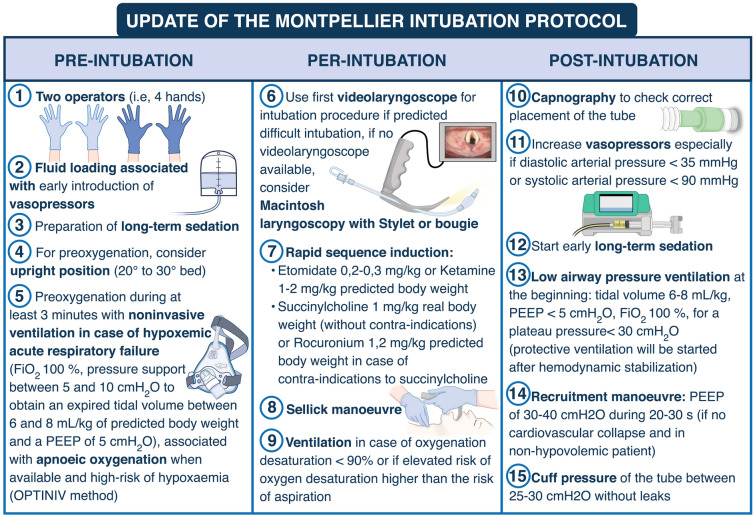
Tracheal intubation in the critically ill is associated with serious complications, mainly cardiovascular collapse and severe hypoxemia. In this narrative review, we present an update of interventions aiming to decrease these complications. MACOCHA is a simple score that helps to identify patients at risk of difficult intubation in the intensive care unit (ICU). Preoxygenation combining the use of inspiratory support and positive end-expiratory pressure should remain the standard method for preoxygenation of hypoxemic patients. Apneic oxygenation using high-flow nasal oxygen may be supplemented, to prevent further hypoxemia during tracheal intubation. Face mask ventilation after rapid sequence induction may also be used to prevent hypoxemia, in selected patients without high-risk of aspiration. Hemodynamic optimization and management are essential before, during and after the intubation procedure. All these elements can be integrated in a bundle. An airway management algorithm should be adopted in each ICU and adapted to the needs, situation and expertise of each operator. Videolaryngoscopes should be used by experienced operators.
Keywords: Airway; Complications; Intubation; Videolaryngoscope; Videolaryngoscopy.
© 2022. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
SJ Jaber reports receiving consulting fees from Drager, Medtronic, Mindray, Fresenius, Baxter, and Fisher & Paykel. ADJ reports receiving remuneration for presentations from Medtronic, Drager and Fisher & Paykel. OR reports receiving research grant from Hamilton Medical AG, speaker fees from Hamilton Medical AG, Fisher & Paykel, Aerogen Ltd and Ambu, and non-financial research support from Timpel. No potential conflict of interest relevant to this article was reported for the other authors.
Figures
Comment in
-
Analgesia as part of the orotracheal intubation induction sequence.Intensive Care Med. 2022 Dec;48(12):1833-1834. doi: 10.1007/s00134-022-06886-9. Epub 2022 Oct 4. Intensive Care Med. 2022. PMID: 36194259 No abstract available.
References
-
- Lascarrou JB, Boisrame-Helms J, Bailly A, Le Thuaut A, Kamel T, Mercier E, Ricard JD, Lemiale V, Colin G, Mira JP, Meziani F, Messika J, Dequin PF, Boulain T, Azoulay E, Champigneulle B, Reignier J. Video laryngoscopy vs direct laryngoscopy on successful first-pass orotracheal intubation among ICU patients: a randomized clinical trial. JAMA. 2017;317:483–493. doi: 10.1001/jama.2016.20603. - DOI - PubMed
-
- Roux D, Reignier J, Thiery G, Boyer A, Hayon J, Souweine B, Papazian L, Mercat A, Bernardin G, Combes A, Chiche JD, Diehl JL, du Cheyron D, L'Her E, Perrotin D, Schneider F, Thuong M, Wolff M, Zeni F, Dreyfuss D, Ricard JD. Acquiring procedural skills in ICUs: a prospective multicenter study*. Crit Care Med. 2014;42:886–895. doi: 10.1097/CCM.0000000000000049. - DOI - PubMed
-
- Martin M, Decamps P, Seguin A, Garret C, Crosby L, Zambon O, Miailhe AF, Canet E, Reignier J, Lascarrou JB. Nationwide survey on training and device utilization during tracheal intubation in French intensive care units. Ann Intensive Care. 2020;10:2. doi: 10.1186/s13613-019-0621-9. - DOI - PMC - PubMed
-
- Jaber S, Amraoui J, Lefrant J-Y, Arich C, Cohendy R, Landreau L, Calvet Y, Capdevila X, Mahamat A, Eledjam J-J. Clinical practice and risk factors for immediate complications of endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Crit Care Med. 2006;34:2355–2361. doi: 10.1097/01.CCM.0000233879.58720.87. - DOI - PubMed
-
- De Jong A, Molinari N, Terzi N, Mongardon N, Arnal JM, Guitton C, Allaouchiche B, Paugam-Burtz C, Constantin JM, Lefrant JY, Leone M, Papazian L, Asehnoune K, Maziers N, Azoulay E, Pradel G, Jung B, Jaber S. Early identification of patients at risk for difficult intubation in the intensive care unit: development and validation of the MACOCHA score in a multicenter cohort study. Am J Respir Crit Care Med. 2013;187:832–839. doi: 10.1164/rccm.201210-1851OC. - DOI - PubMed
