

Venting during venoarterial extracorporeal membrane oxygenation
- PMID: 35986750
- PMCID: PMC10050067
- DOI: 10.1007/s00392-022-02069-0
Venting during venoarterial extracorporeal membrane oxygenation
Abstract
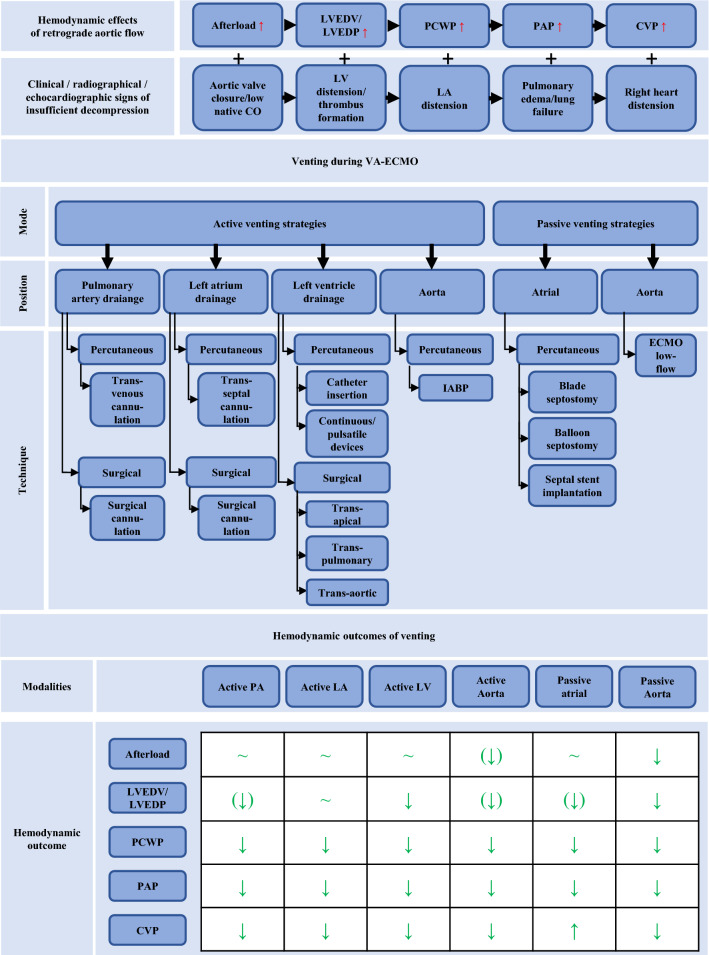
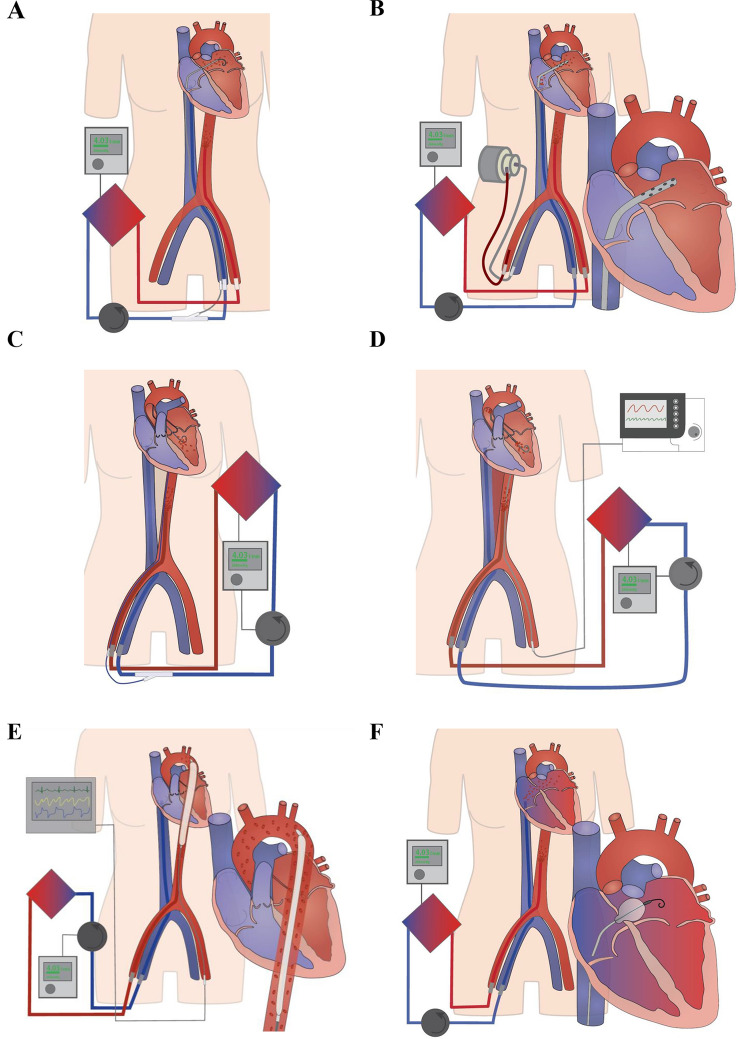
Cardiogenic shock and cardiac arrest contribute pre-dominantly to mortality in acute cardiovascular care. Here, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) has emerged as an established therapeutic option for patients suffering from these life-threatening entities. VA-ECMO provides temporary circulatory support until causative treatments are effective and enables recovery or serves as a bridging strategy to surgical ventricular assist devices, heart transplantation or decision-making. However, in-hospital mortality rate in this treatment population is still around 60%. In the recently published ARREST trial, VA-ECMO treatment lowered mortality rate in patients with ongoing cardiac arrest due to therapy refractory ventricular fibrillation compared to standard advanced cardiac life support in selected patients. Whether VA-ECMO can reduce mortality compared to standard of care in cardiogenic shock has to be evaluated in the ongoing prospective randomized studies EURO-SHOCK (NCT03813134) and ECLS-SHOCK (NCT03637205). As an innate drawback of VA-ECMO treatment, the retrograde aortic flow could lead to an elevation of left ventricular (LV) afterload, increase in LV filling pressure, mitral regurgitation, and elevated left atrial pressure. This may compromise myocardial function and recovery, pulmonary hemodynamics-possibly with concomitant pulmonary congestion and even lung failure-and contribute to poor outcomes in a relevant proportion of treated patients. To overcome these detrimental effects, a multitude of venting strategies are currently engaged for both preventive and emergent unloading. This review aims to provide a comprehensive and structured synopsis of existing venting modalities and their specific hemodynamic characteristics. We discuss in detail the available data on outcome categories and complication rates related to the respective venting option.
Keywords: Cardiogenic shock; Decompression; ECMELLA; IABP; Impella; Percutaneous microaxial pump; Unloading; VA-ECMO; Venting.
© 2022. The Author(s).
Conflict of interest statement
Martin Orban has received speaker honoraria from Abbott Medical, AstraZeneca, Abiomed, Bayer vital, Biotronik, Bristol-Myers Squibb, CytoSorbents, Daiichi Sankyo Deutschland, Edwards Lifesciences Services, Sedana Medical, outside the submitted work. The other authors declare no conflict of interests. Andreas Schäfer has received lecture fees and research support from Abiomed.
Figures
References
-
- Yannopoulos D, Bartos J, Raveendran G, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020;396:1807–1816. doi: 10.1016/S0140-6736(20)32338-2. - DOI - PMC - PubMed
-
- Banning AS, Adriaenssens T, Berry C, et al. Veno-arterial extracorporeal membrane oxygenation (ECMO) in patients with cardiogenic shock: rationale and design of the randomised, multicentre, open-label EURO SHOCK trial. EuroIntervention. 2021;16:e1227–e1236. doi: 10.4244/EIJ-D-20-01076. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
