

Impact of site of occlusion in proximal splenic artery embolisation for blunt splenic trauma
- PMID: 35986797
- PMCID: PMC9391208
- DOI: 10.1186/s42155-022-00315-0
Impact of site of occlusion in proximal splenic artery embolisation for blunt splenic trauma
Abstract
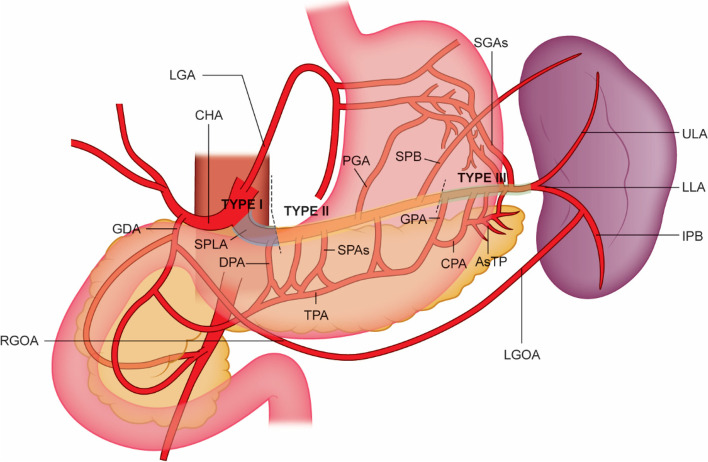
Background: Proximal splenic artery embolisation (PSAE) can be performed in stable patients with Association for the Surgery of Trauma (AAST) grade III-V splenic injury. PSAE reduces splenic perfusion but maintains viability of the spleen and pancreas via the collateral circulation. The hypothesized ideal location is between the dorsal pancreatic artery (DPA) and great pancreatic artery (GPA). This study compares the outcomes resulting from PSAE embolisation in different locations along the splenic artery.
Materials and methods: Retrospective review was performed of PSAE for blunt splenic trauma (2015-2020). Embolisation locations were divided into: Type I, proximal to DPA; Type II, DPA-GPA; Type III, distal to GPA. Fifty-eight patients underwent 59 PSAE: Type I (7); Type II (27); Type III (25). Data was collected on technical and clinical success, post-embolisation pancreatitis and splenic perfusion. Statistical significance was assessed using a chi-squared test.
Results: Technical success was achieved in 100% of cases. Clinical success was 100% for Type I/II embolisation and 88% for Type III: one patient underwent reintervention and two had splenectomies for ongoing instability. Clinical success was significantly higher in Type II embolisation compared to Type III (p = 0.02). No episodes of pancreatitis occurred post-embolisation. Where post-procedural imaging was obtained, splenic perfusion remained 100% in Type I and II embolisation and 94% in Type III. Splenic perfusion was significantly higher in the theorized ideal Type II group compared to Type I and III combined (p = 0.01).
Conclusion: The results support the proposed optimal embolisation location as being between the DPA and GPA.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources