

Antihypertensive and Statin Medication Adherence Among Medicare Beneficiaries
- PMID: 35987557
- PMCID: PMC10851130
- DOI: 10.1016/j.amepre.2022.02.019
Antihypertensive and Statin Medication Adherence Among Medicare Beneficiaries
Abstract
Introduction: Medication adherence is important for optimal management of chronic conditions, including hypertension and hypercholesterolemia. This study describes adherence to antihypertensive and statin medications, individually and collectively, and examines variation in adherence by demographic and geographic characteristics.
Methods: The 2017 prescription drug event data for beneficiaries with Medicare Part D coverage were assessed. Beneficiaries with a proportion of days covered ≥80% were considered adherent. Adjusted prevalence ratios were estimated to quantify the associations between demographic and geographic characteristics and adherence. Adherence estimates were mapped by county of residence using a spatial empirical Bayesian smoothing technique to enhance stability. Analyses were conducted in 2019‒2021.
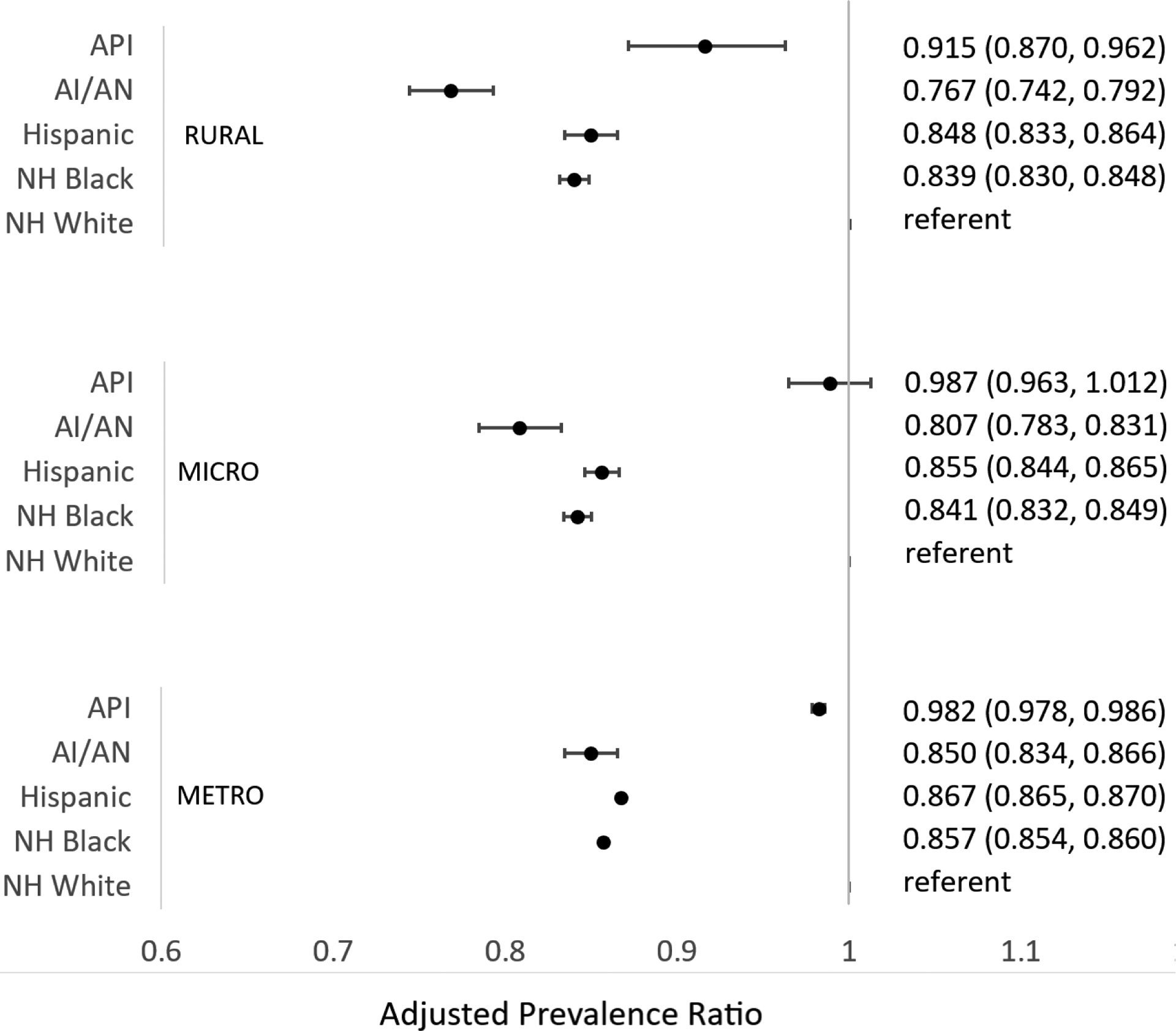
Results: Among the 22.5 million beneficiaries prescribed antihypertensive medications, 77.1% were adherent; among the 16.1 million prescribed statin medications, 81.9% were adherent; and among the 13.5 million prescribed antihypertensive and statin medications, 70.3% were adherent to both. Adherence varied by race/ethnicity: American Indian/Alaska Native (adjusted prevalence ratio=0.83, 95% confidence limit=0.82, 0.842), Hispanic (adjusted prevalence ratio=0.90, 95% confidence limit=0.90, 0.91), and non-Hispanic Black (adjusted prevalence ratio=0.87, 95% confidence limit=0.86, 0.87) beneficiaries were less likely to be adherent than non-Hispanic White beneficiaries. County-level adherence ranged across the U.S. from 25.7% to 88.5% for antihypertensive medications, from 36.0% to 93.8% for statin medications, and from 20.8% to 92.9% for both medications combined and tended to be the lowest in the southern U.S.
Conclusions: This study highlights opportunities for efforts to remove barriers and support medication adherence, especially among racial/ethnic minority groups and within the regions at greatest risk for adverse cardiovascular outcomes.
Published by Elsevier Inc.
Conflict of interest statement
Figures

Similar articles
-
Vital Signs: Disparities in Antihypertensive Medication Nonadherence Among Medicare Part D Beneficiaries - United States, 2014.MMWR Morb Mortal Wkly Rep. 2016 Sep 16;65(36):967-76. doi: 10.15585/mmwr.mm6536e1. MMWR Morb Mortal Wkly Rep. 2016. PMID: 27632693
-
Association between dispensing channel and medication adherence among medicare beneficiaries taking medications to treat diabetes, high blood pressure, or high blood cholesterol.J Manag Care Spec Pharm. 2014 Aug;20(8):851-61. doi: 10.18553/jmcp.2014.20.8.851. J Manag Care Spec Pharm. 2014. PMID: 25062079 Free PMC article.
-
Comparison of statin adherence among beneficiaries in MA-PD plans versus PDPs.J Manag Care Pharm. 2012 Mar;18(2):106-15. doi: 10.18553/jmcp.2012.18.2.106. J Manag Care Pharm. 2012. PMID: 22380470 Free PMC article.
-
Assessing the association between medication adherence, as defined in quality measures, and disease-state control, health care utilization, and costs in a retrospective database analysis of Medicare supplemental beneficiaries using statin medications.J Manag Care Spec Pharm. 2020 Dec;26(12):1529-1537. doi: 10.18553/jmcp.2020.26.12.1529. J Manag Care Spec Pharm. 2020. PMID: 33251989 Free PMC article.
-
Behavioral and Pharmacotherapy Weight Loss Interventions to Prevent Obesity-Related Morbidity and Mortality in Adults: An Updated Systematic Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Sep. Report No.: 18-05239-EF-1. PMID: 30354042 Free Books & Documents. Review.
Cited by
-
Statin Twitter: Human and Automated Bot Contributions, 2010 to 2022.J Am Heart Assoc. 2024 Apr 2;13(7):e032678. doi: 10.1161/JAHA.123.032678. Epub 2024 Mar 27. J Am Heart Assoc. 2024. PMID: 38533942 Free PMC article.
-
Estimating the economic impact of blister-packaging on medication adherence and health care costs for a Medicare Advantage health plan.J Manag Care Spec Pharm. 2024 Dec;30(12):1442-1454. doi: 10.18553/jmcp.2024.24179. Epub 2024 Sep 11. J Manag Care Spec Pharm. 2024. PMID: 39258999 Free PMC article.
-
Influenza vaccination and use of lipid lowering therapies in adults with atherosclerotic cardiovascular disease: An analysis of the Behavioral Risk Factor Surveillance System (BRFSS).Am Heart J. 2024 Feb;268:1-8. doi: 10.1016/j.ahj.2023.11.007. Epub 2023 Nov 11. Am Heart J. 2024. PMID: 37956919 Free PMC article.
-
Suitability of Measures of Pharmacy-Based Medication Adherence for Routine Clinical Use Among Patients with Chronic Diseases: A Systematic Review.Patient Prefer Adherence. 2025 Jan 30;19:265-278. doi: 10.2147/PPA.S492461. eCollection 2025. Patient Prefer Adherence. 2025. PMID: 39901904 Free PMC article. Review.
-
Continuity of Medication Use by US Adults With Diabetes, 2005-2019.JAMA Netw Open. 2023 Jan 3;6(1):e2253562. doi: 10.1001/jamanetworkopen.2022.53562. JAMA Netw Open. 2023. PMID: 36716032 Free PMC article.
References
-
- Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021;143(8):e254–e743. - PubMed
-
- Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018;71(6):1269–1324. - PubMed
-
- Grundy SM, Stone NJ, Bailey AL, Beam C, Birtcher KK, Blumenthal RS, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019;139(25):e1082–e1143. - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
