

High fluoroquinolone resistance proportions among multidrug-resistant tuberculosis driven by dominant L2 Mycobacterium tuberculosis clones in the Mumbai Metropolitan Region
- PMID: 35989319
- PMCID: PMC9394022
- DOI: 10.1186/s13073-022-01076-0
High fluoroquinolone resistance proportions among multidrug-resistant tuberculosis driven by dominant L2 Mycobacterium tuberculosis clones in the Mumbai Metropolitan Region
Abstract
Background: Multidrug-resistant (MDR) Mycobacterium tuberculosis complex (MTBC) strains are a serious health problem in India, also contributing to one-fourth of the global MDR tuberculosis (TB) burden. About 36% of the MDR MTBC strains are reported fluoroquinolone (FQ) resistant leading to high pre-extensively drug-resistant (pre-XDR) and XDR-TB (further resistance against bedaquiline and/or linezolid) rates. Still, factors driving the MDR/pre-XDR epidemic in India are not well defined.
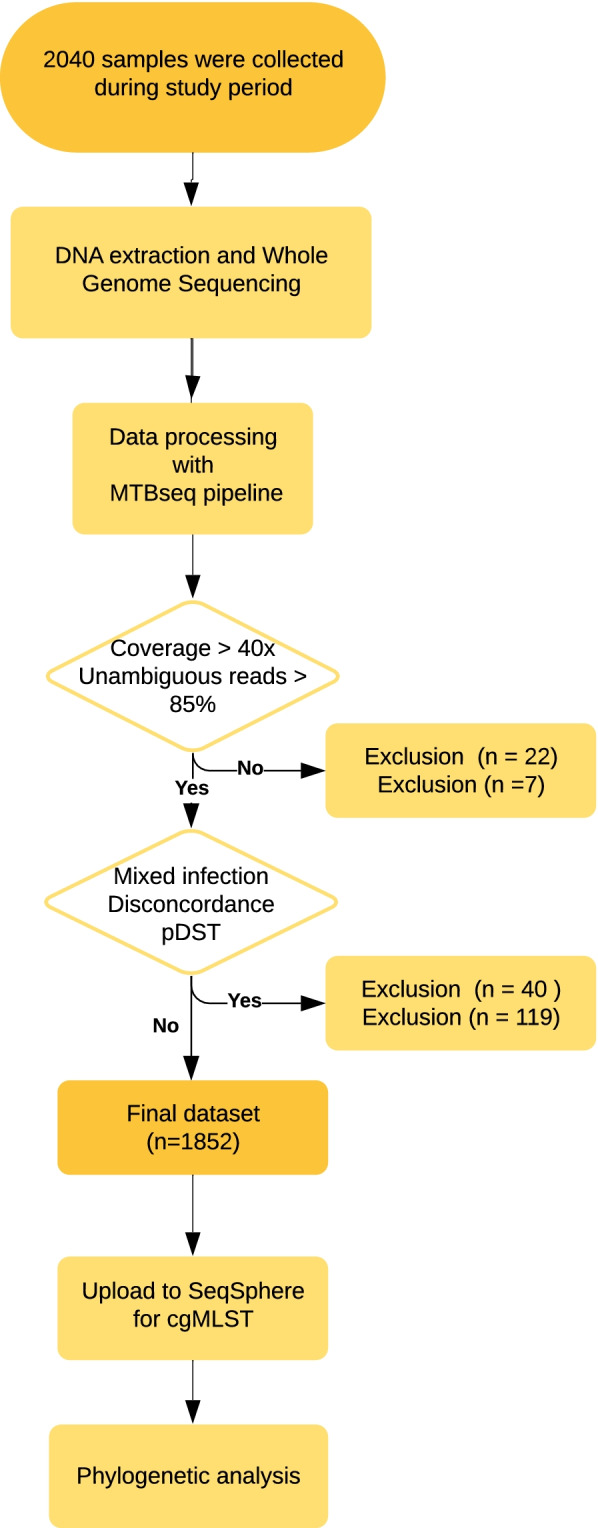
Methods: In a retrospective study, we analyzed 1852 consecutive MTBC strains obtained from patients from a tertiary care hospital laboratory in Mumbai by whole genome sequencing (WGS). Univariate and multivariate statistics was used to investigate factors associated with pre-XDR. Core genome multi locus sequence typing, time scaled haplotypic density (THD) method and homoplasy analysis were used to analyze epidemiological success, and positive selection in different strain groups, respectively.
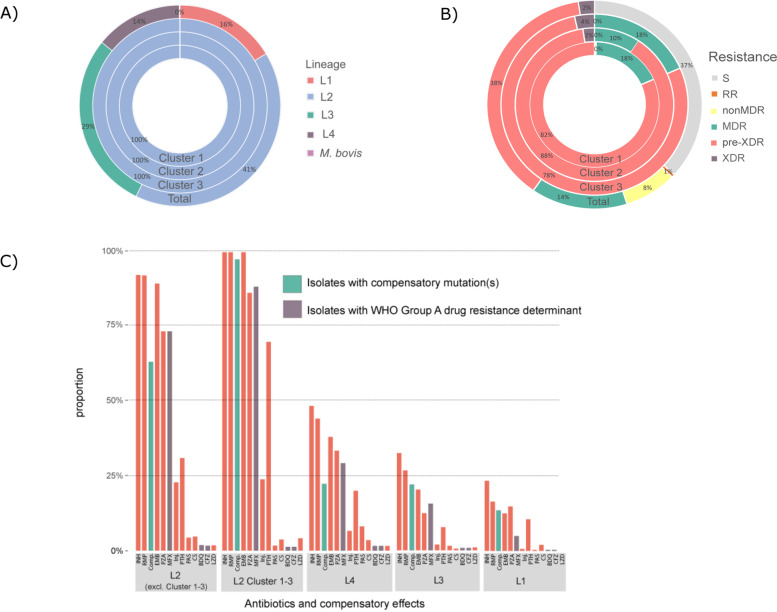
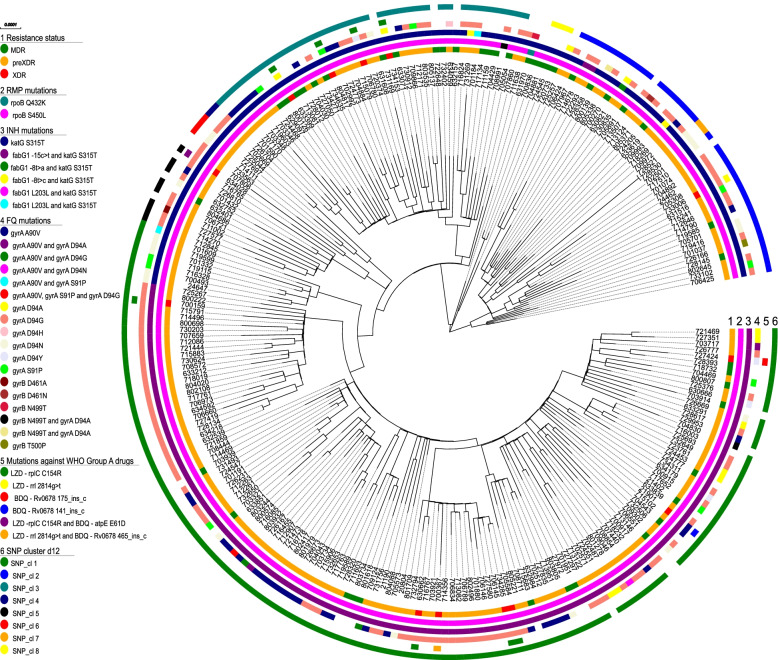
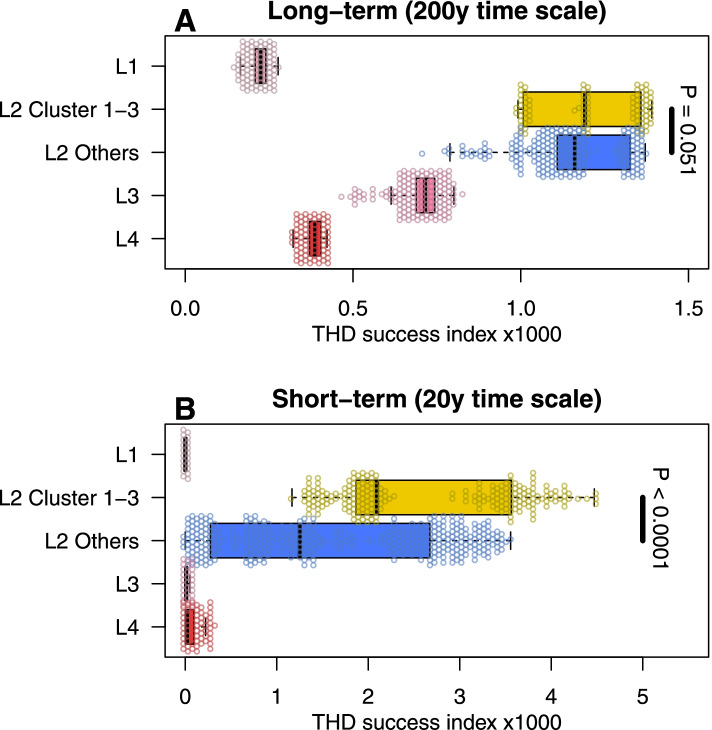
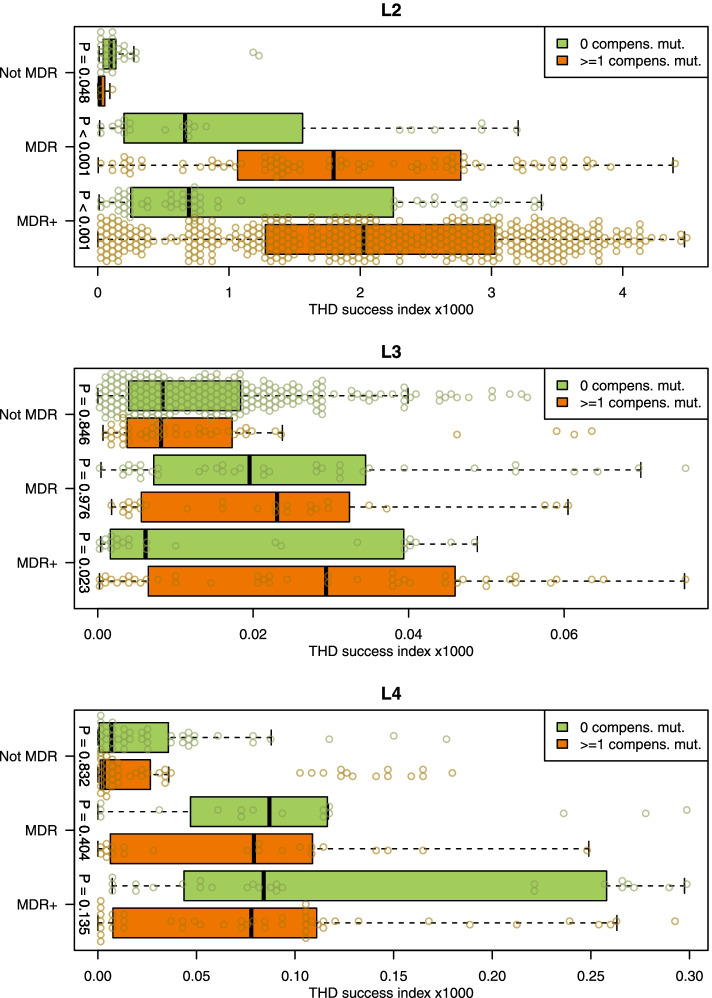
Results: In total, 1016 MTBC strains were MDR, out of which 703 (69.2%) were pre-XDR and 45 (4.4%) were XDR. Cluster rates were high among MDR (57.8%) and pre-XDR/XDR (79%) strains with three dominant L2 (Beijing) strain clusters (Cl 1-3) representing half of the pre-XDR and 40% of the XDR-TB cases. L2 strains were associated with pre-XDR/XDR-TB (P < 0.001) and, particularly Cl 1-3 strains, had high first-line and FQ resistance rates (81.6-90.6%). Epidemic success analysis using THD showed that L2 strains outperformed L1, L3, and L4 strains in short- and long-term time scales. More importantly, L2 MDR and MDR + strains had higher THD success indices than their not-MDR counterparts. Overall, compensatory mutation rates were highest in L2 strains and positive selection was detected in genes of L2 strains associated with drug tolerance (prpB and ppsA) and virulence (Rv2828c). Compensatory mutations in L2 strains were associated with a threefold increase of THD indices, suggesting improved transmissibility.
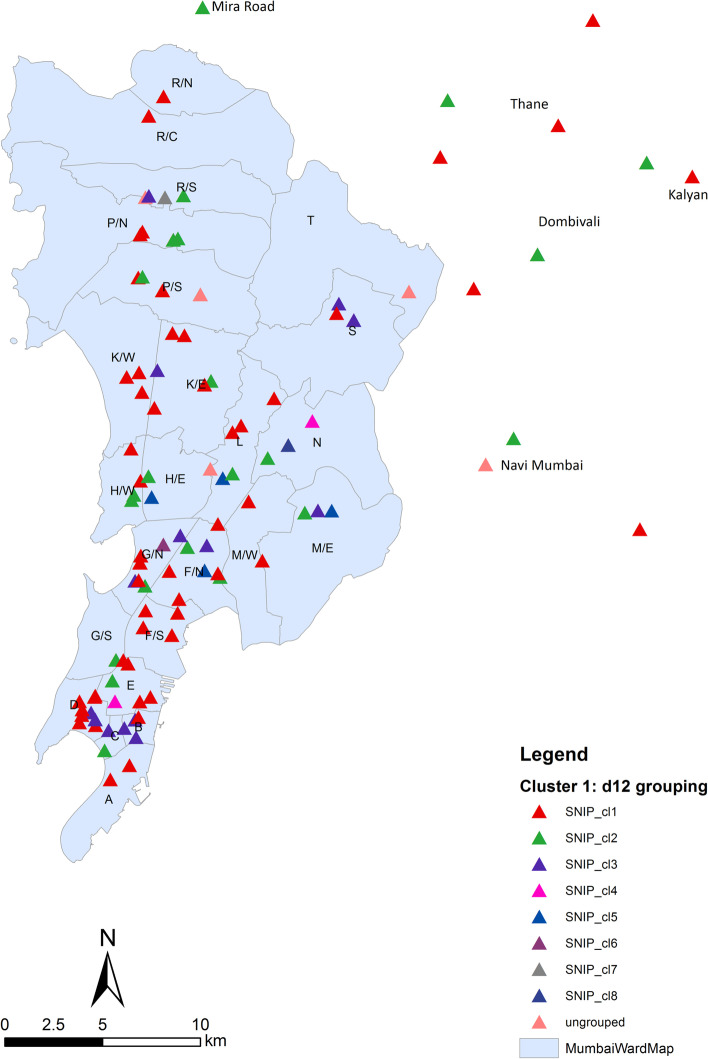
Conclusions: Our data indicate a drastic increase of FQ resistance, as well as emerging bedaquiline resistance which endangers the success of newly endorsed MDR-TB treatment regimens. Rapid changes in treatment and control strategies are required to contain transmission of highly successful pre-XDR L2 strains in the Mumbai Metropolitan region but presumably also India-wide.
Keywords: Fluoroquinolone resistance; India; Pre-XDR/XDR-TB; Multidrug-resistant TB; Pre-XDR/XDR-TB transmission; Resistant TB; Transmission success; Tuberculosis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- WHO | Global tuberculosis report 2020 [Internet]. WHO. World Health Organization; [cited 2020 Nov 4]. Available from: http://www.who.int/tb/publications/global_report/en/
-
- World Health Organization . Global Tuberculosis Report 2019. S.l.: World Health Organization; 2019.
-
- Dheda K, Gumbo T, Maartens G, Dooley KE, McNerney R, Murray M, et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir Med. 2017;5:291–360. doi: 10.1016/S2213-2600(17)30079-6. - DOI - PubMed
-
- World Health Organization. Meeting report of the WHO expert consultation on the definition of extensively drug-resistant tuberculosis [Internet]. Geneva, Switzerland; 2021. Available from: https://www.who.int/publications-detail-redirect/meeting-report-of-the-w...
