

Impact of high frequency stimulation to confirm a complete box isolation in catheter ablation of non-paroxysmal atrial fibrillation
- PMID: 35989415
- PMCID: PMC9826345
- DOI: 10.1111/pace.14582
Impact of high frequency stimulation to confirm a complete box isolation in catheter ablation of non-paroxysmal atrial fibrillation
Abstract
Introduction: Pulmonary vein (PV) isolation (PVI) including the left atrial posterior wall (LAPW) (Box-PVI) is proposed as an additional strategy for non-paroxysmal atrial fibrillation (NPAF), however, the efficacy remains controversial. The more reliable and durable the Box-PVI we can create, the better the rhythm outcomes might be than with a conventional PVI alone. This study focused on the potential exit conduction of the box lesion and investigated whether the conventional Box-PVI would be sufficient.
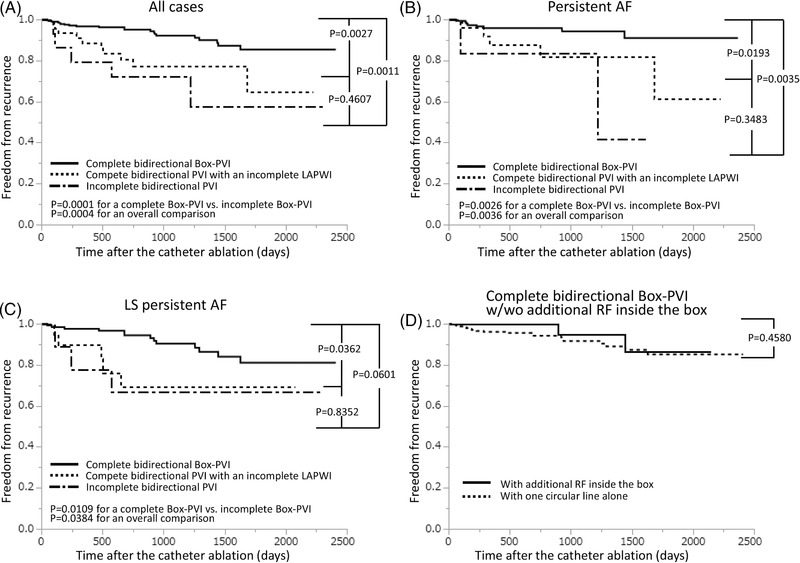
Methods and results: We enrolled 350 consecutive patients with NPAF that underwent a conventional encircling Box-PVI and examined whether latent exit conduction and dormant "exit" conduction independently remained on the LAPW and in the PVs using high frequency stimulation (HFS) and an adenosine triphosphate (ATP) injection. All electrograms inside the box lesion were eliminated in all cases, however, HFS inside the box propagated outward in 23 cases (6.6%) without any exit conduction by conventional burst stimulation, and 24 cases (6.9%) exhibited only dormant "exit" conduction of the LAPW. Additional ablation where positive HFSs were observed created a complete bidirectional Box-PVI in 43 (41.3%) of the cases without a first pass Box-PVI. The recurrence rates depended on the groups classified according to the HFS response.
Conclusion: HFS delivered with an ATP injection on the LAPW and in the PVs following a Box-PVI could not only elucidate true exit block but also identified possible incomplete lesions or connections outside the ablation line, whose elimination could achieve a complete Box-PVI leading to a better rhythm outcome.
Keywords: adenosine triphosphate; box isolation; dormant conduction; exit block; pulmonary vein isolation.
© 2022 The Authors. Pacing and Clinical Electrophysiology published by Wiley Periodicals LLC.
Conflict of interest statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not‐for‐profit sectors. All the authors have no conflicts to disclose.
Figures





References
-
- Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659‐666 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
