

Real-World Effectiveness of Beta-Blockers versus Other Antihypertensives in Reducing All-Cause Mortality and Cardiovascular Events
- PMID: 35989866
- PMCID: PMC9356871
- DOI: 10.1155/2022/6124559
Real-World Effectiveness of Beta-Blockers versus Other Antihypertensives in Reducing All-Cause Mortality and Cardiovascular Events
Abstract
Aim: The aim of the study was to compare the effectiveness of beta-blockers with other antihypertensive classes in reducing all-cause mortality, cardiovascular-related mortality and the risk of cerebrocardiovascular events.
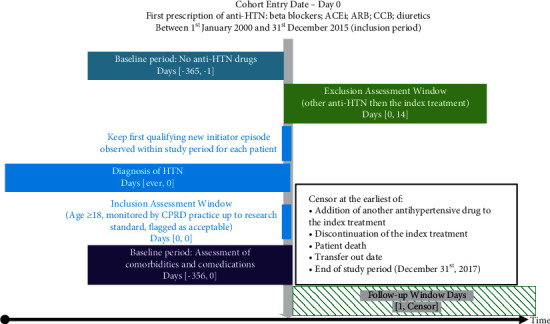
Methods: This noninterventional study was conducted within the UK Clinical Practice Research Datalink. Hypertensive patients who initiated antihypertensive monotherapy were allocated to one of five cohorts: beta-blockers; angiotensin-converting enzyme inhibitors (ACEi); angiotensin II receptor blockers (ARB); calcium channel blockers (CCB); and diuretics. Differences in outcomes were assessed using Cox proportional hazard models with competing risks.
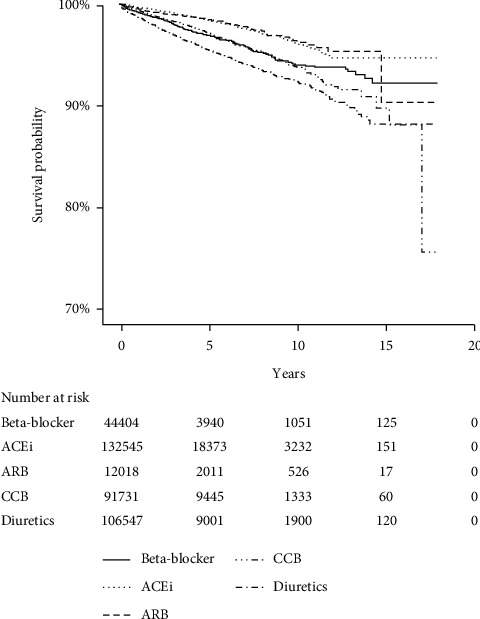
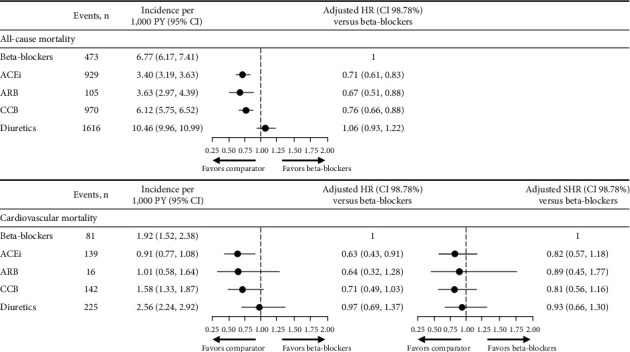
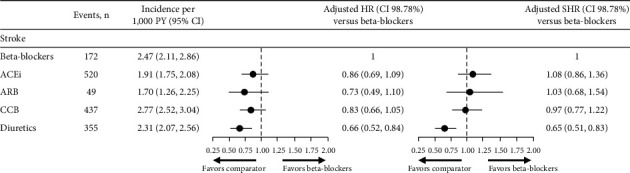
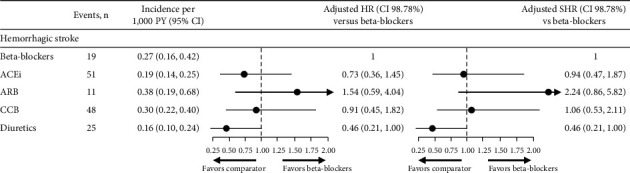
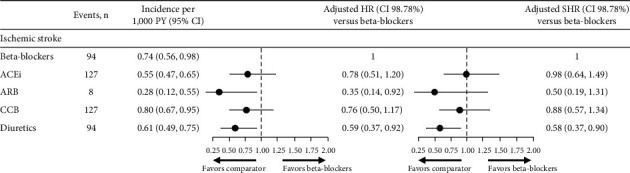
Results: A total of 44,404 patients were prescribed beta-blockers (75% atenolol), 132,545 ACEi, 12,018 ARB, 91,731 CCB, and 106,547 diuretics. At baseline, patients in the beta-blocker cohort presented more frequently with angina, arrhythmia, and atrial fibrillation. The risk of all-cause mortality was lower for those treated with ACEi, ARB, and CCB, and no difference was observed compared with diuretics (adjusted hazard ratio versus beta-blockers (98.75% CI), for ACEi 0.71 (0.61, 0.83), ARB 0.67 (0.51, 0.88), CCB 0.76 (0.66, 0.88), diuretics 1.06 (0.93, 1.22)). No differences were seen in the risk of cardiovascular mortality for patients treated with beta-blockers, ARB, CCB, and diuretics, while a lower risk in patients treated with ACEi was observed (ACEi 0.63 (0.43, 0.91), ARB 0.64 (0.32, 1.28), CCB 0.71 (0.49, 1.03), diuretics 0.97 (0.69, 1.37)).
Conclusions: These data add to the limited pool of evidence from real-world studies exploring the effectiveness of beta-blockers versus other antihypertensive classes. Discrepancies to previously published studies might be partly explained by differences in the selected populations and in the follow-up time.
Copyright © 2022 Caroline Foch et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Renin-Angiotensin-Aldosterone System-based Antihypertensive Agents and the Risk of Colorectal Cancer Among Medicare Beneficiaries.Epidemiology. 2019 Nov;30(6):867-875. doi: 10.1097/EDE.0000000000001065. Epidemiology. 2019. PMID: 31348009 Free PMC article.
-
[Assessment of antihypertensive monotherapies effectiveness by home blood pressure self-measurement in hypertensive patients].Ann Cardiol Angeiol (Paris). 2012 Jun;61(3):218-23. doi: 10.1016/j.ancard.2012.05.002. Epub 2012 May 23. Ann Cardiol Angeiol (Paris). 2012. PMID: 22695025 French.
-
Analysis of Dual Combination Therapies Used in Treatment of Hypertension in a Multinational Cohort.JAMA Netw Open. 2022 Mar 1;5(3):e223877. doi: 10.1001/jamanetworkopen.2022.3877. JAMA Netw Open. 2022. PMID: 35323951 Free PMC article.
-
Role of antihypertensive therapy with angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers in combination with calcium channel blockers for stroke prevention.J Am Pharm Assoc (2003). 2010 Sep-Oct;50(5):e116-25. doi: 10.1331/JAPhA.2010.09234. J Am Pharm Assoc (2003). 2010. PMID: 20833609 Review.
-
Effects of blood pressure-lowering treatment on cardiovascular outcomes and mortality: 14 - effects of different classes of antihypertensive drugs in older and younger patients: overview and meta-analysis.J Hypertens. 2018 Aug;36(8):1637-1647. doi: 10.1097/HJH.0000000000001777. J Hypertens. 2018. PMID: 29847487 Review.
References
-
- Mancia G., Fagard R., Narkiewicz K., et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European society of hypertension (ESH) and of the European society of cardiology (ESC) Journal of Hypertension . 2013;31(7):1281–1357. doi: 10.1097/01.hjh.0000431740.32696.cc. - DOI - PubMed
-
- The National Institute for Health and Care Excellence (NICE) Hypertension in adults: diagnosis and management 2019. 2021. https://www.nice.org.uk/guidance/ng136 . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical