

Short- and long-term mortality of subarachnoid hemorrhage according to hospital volume and severity using a nationwide multicenter registry study
- PMID: 35989903
- PMCID: PMC9389169
- DOI: 10.3389/fneur.2022.952794
Short- and long-term mortality of subarachnoid hemorrhage according to hospital volume and severity using a nationwide multicenter registry study
Abstract
Introduction: Recent improvements in treatment for subarachnoid hemorrhage (SAH) have decreased the mortality rates; however, the outcomes of SAH management are dependent on many other factors. In this study, we used nationwide, large-scale, observational data to investigate short- and long-term mortality rates after SAH treatment and the influence of patient severity and hospital volume.
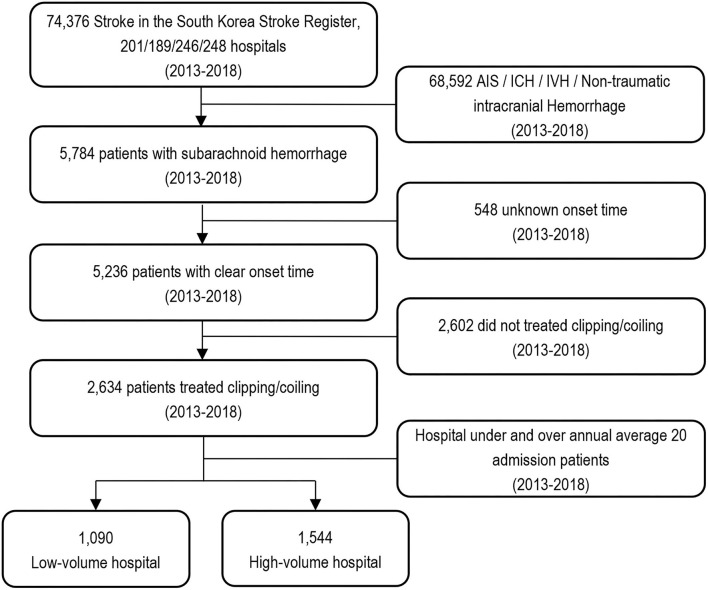
Patients and methods: We selected patients with SAH treated with clipping and coiling from the South Korean Acute Stroke Assessment Registry. High- and low-volume hospitals performed ≥20 clipping and coiling procedures and <20 clipping and coiling procedures per year, respectively. Short- and long-term mortality were tracked using data from the Health Insurance Review and Assessment Service.
Results: Among 2,634 patients treated using clipping and coiling, 1,544 (58.6%) and 1,090 (41.4%) were hospitalized in high- and low-volume hospitals, respectively, and 910 (34.5%) and 1,724 (65.5%) were treated with clipping and coiling, respectively. Mortality rates were 13.5, 14.4, 15.2, and 16.1% at 3 months, 1, 2, and 4 years, respectively. High-volume hospitals had a significantly lower 3-month mortality rate. Patients with mild clinical status had a significantly lower 3-month mortality rate in high-volume hospitals than in low-volume hospitals. Patients with severe clinical status had significantly lower 1- and 2-year mortality rates in high-volume hospitals than in low-volume hospitals.
Conclusion: Short- and long-term mortality in patients with SAH differed according to hospital volume. In the modern endovascular era, clipping and coiling can lead to better outcomes in facilities with high stroke-care capabilities.
Keywords: hospital volume; long-term outcomes; mortality; short-term outcomes; subarachnoid hemorrhage.
Copyright © 2022 Park, Lee, Heo, Han, Lee, Hong, Lee, Lee and Oh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


Similar articles
-
Short and Long-term Outcomes of Subarachnoid Hemorrhage Treatment according to Hospital Volume in Korea: a Nationwide Multicenter Registry.J Korean Med Sci. 2021 Jun 7;36(22):e146. doi: 10.3346/jkms.2021.36.e146. J Korean Med Sci. 2021. PMID: 34100560 Free PMC article.
-
Effects of case volume and comprehensive stroke center capabilities on patient outcomes of clipping and coiling for subarachnoid hemorrhage.J Neurosurg. 2020 Mar 13;134(3):929-939. doi: 10.3171/2019.12.JNS192584. Print 2021 Mar 1. J Neurosurg. 2020. PMID: 32168489
-
No Disparity in Outcomes Between Surgical Clipping and Endovascular Coiling After Aneurysmal Subarachnoid Hemorrhage.World Neurosurg. 2018 Dec;120:e318-e325. doi: 10.1016/j.wneu.2018.08.060. Epub 2018 Sep 21. World Neurosurg. 2018. PMID: 30244185
-
In-hospital mortality and poor outcome after surgical clipping and endovascular coiling for aneurysmal subarachnoid hemorrhage using nationwide databases: a systematic review and meta-analysis.Neurosurg Rev. 2020 Apr;43(2):655-667. doi: 10.1007/s10143-019-01096-2. Epub 2019 Apr 2. Neurosurg Rev. 2020. PMID: 30941595
-
Neuropsychological function after endovascular and neurosurgical treatment of subarachnoid hemorrhage: a systematic review and meta-analysis.J Neurosurg. 2018 Mar;128(3):768-776. doi: 10.3171/2016.11.JNS162055. Epub 2017 Apr 14. J Neurosurg. 2018. PMID: 28409729
Cited by
-
Subarachnoid Hemorrhage in Patients with SARS-CoV-2 Infection: Protocol for A Scoping Review.Brain Sci. 2022 Sep 30;12(10):1327. doi: 10.3390/brainsci12101327. Brain Sci. 2022. PMID: 36291263 Free PMC article.
-
Comparison of long-term clinical outcome after endovascular versus neurosurgical treatment of ruptured intracranial anterior circulation aneurysms: A single-centre experience.Brain Spine. 2024 Jul 15;4:102902. doi: 10.1016/j.bas.2024.102902. eCollection 2024. Brain Spine. 2024. PMID: 39155957 Free PMC article.
-
Pharmacotherapy in SAH: Clinical Trial Lessons.CNS Neurol Disord Drug Targets. 2024;23(11):1308-1319. doi: 10.2174/0118715273251761231127095039. CNS Neurol Disord Drug Targets. 2024. PMID: 38243987 Review.
-
Results of an Online Survey on Intensive Care Management of Patients with Aneurysmal Subarachnoid Hemorrhage in German-Speaking Countries.J Clin Med. 2024 Dec 13;13(24):7614. doi: 10.3390/jcm13247614. J Clin Med. 2024. PMID: 39768538 Free PMC article.
-
Distinct Gut Microbiota Profiles in Unruptured and Ruptured Intracranial Aneurysms: Focus on Butyrate-Producing Bacteria.J Clin Med. 2025 May 16;14(10):3488. doi: 10.3390/jcm14103488. J Clin Med. 2025. PMID: 40429482 Free PMC article.
References
LinkOut - more resources
Full Text Sources