

Bridging intravenous thrombolysis in patients with atrial fibrillation
- PMID: 35989924
- PMCID: PMC9382124
- DOI: 10.3389/fneur.2022.945338
Bridging intravenous thrombolysis in patients with atrial fibrillation
Abstract
Background and purpose: 40% of acute ischemic stroke patients treated by mechanical thrombectomy (MT) have a clinical history of atrial fibrillation (AF). The safety of bridging intravenous thrombolysis (IVT) (MT + IVT) is currently being discussed. We aimed to analyze the interaction between oral anticoagulation (OAC) status or AF with bridging IVT, regarding the occurrence of symptomatic intracranial hemorrhage (sICH) and functional outcome.
Materials and methods: Multicentric observational cohort study (BEYOND-SWIFT registry) of consecutive patients undergoing MT between 2010 and 2018 (n = 2,941). Multinomial regression models were adjusted for prespecified baseline and plausible pathophysiological covariates identified on a univariate analysis to assess the association of AF and OAC status with sICH and good outcomes (90-day modified Rankin Scale score 0-2).
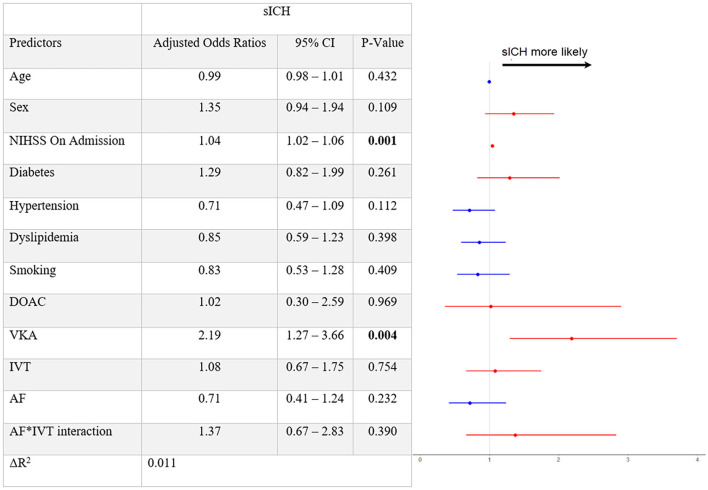
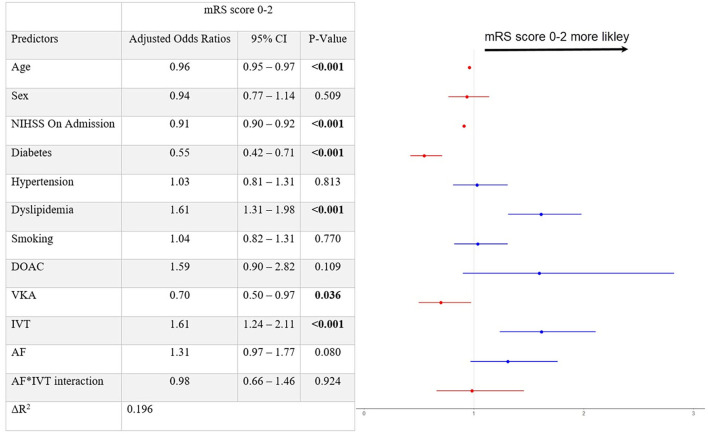
Results: In the total cohort (median age 74, 50.6% women), 1,347 (45.8%) patients had AF. Higher admission National Institutes of Health Stroke Scale (NIHSS) score (aOR 1.04 [95% 1.02-1.06], per point of increase) and prior medication with Vitamin K antagonists (VKA) (aOR 2.19 [95% 1.27-3.66]) were associated with sICH. Neither AF itself (aOR 0.71 [95% 0.41-1.24]) nor bridging IVT (aOR 1.08 [0.67-1.75]) were significantly associated with increased sICH. Receiving bridging IVT (aOR 1.61 [95% 1.24-2.11]) was associated with good 90-day outcome, with no interaction between AF and IVT (p = 0.92).
Conclusion: Bridging IVT appears to be a reasonable clinical option in selected patients with AF. Given the increased sICH risk in patients with VKA, subgroup analysis of the randomized controlled trials should analyze whether patients with VKA might benefit from withholding bridging IVT.
Registration: clinicaltrials.gov; Unique identifier: NCT03496064.
Keywords: atrial fibrillation; intravenous thrombolysis; ischemic stroke; mechanical thrombectomy; oral anticoagulation.
Copyright © 2022 Mujanovic, Kurmann, Dobrocky, Olivé-Gadea, Maegerlein, Pierot, Mendes Pereira, Costalat, Psychogios, Michel, Beyeler, Piechowiak, Seiffge, Mordasini, Arnold, Gralla, Fischer, Kaesmacher, Meinel and the BEYOND-SWIFT Investigators.
Conflict of interest statement
LP reports personal fees from Balt, Phenox, and Microvention outside the submitted work. VM reports personal fees from Medtronic and Stryker during the conduct of this study. PMo reports research support from Siemens, Cerenovus, iSchemaview, Medtronic, and Stryker and is receipt of honoraria and consultation fees from Medtronic, Cerenovus, Phenox, and Microvention. MA reports personal fees from Bayer, Bristol-Myers Squibb, Medtronic, Amgen, Daiichi Sankyo, Nestlé Health Sciences, Boehringer Ingelheim, and Covidien during the conduct of this study. JG is the global coprincipal investigator of the SWIFT DIRECT trial (Solitaire with the Intention for Thrombectomy Plus Intravenous tPA Versus DIRECT Solitaire Stent-Retriever Thrombectomy in Acute Anterior Circulation Stroke; Medtronic), therefore, consultant Medtronic. He receives Swiss National Science Foundation grants for magnetic resonance imaging in stroke. UF reports grants from Medtronic during the conduct of this study; grants from Medtronic; and others from Medtronic, Stryker, and CSL Behring outside the submitted work and his board membership at the Journal of NeuroInterventional Surgery. JK reports grants from the Swiss Academy of Medical Sciences/Bangerter Foundation, Swiss Stroke Society, and Clinical Trial Unit Bern during the conduct of this study. TM reports research support from the Bangerter Rhyner Foundation, the Swiss National Foundation, and the Swiss Heart Foundation. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical