

Development and validation of a prediction nomogram for a 6-month unfavorable prognosis in traumatic brain-injured patients undergoing primary decompressive craniectomy: An observational study
- PMID: 35989929
- PMCID: PMC9382105
- DOI: 10.3389/fneur.2022.944608
Development and validation of a prediction nomogram for a 6-month unfavorable prognosis in traumatic brain-injured patients undergoing primary decompressive craniectomy: An observational study
Abstract
Objective: This study was designed to develop and validate a risk-prediction nomogram to predict a 6-month unfavorable prognosis in patients with traumatic brain-injured (TBI) undergoing primary decompressive craniectomy (DC).
Methods: The clinical data of 391 TBI patients with primary DC who were admitted from 2012 to 2020 were reviewed, from which 274 patients were enrolled in the training group, while 117 were enrolled in the internal validation group, randomly. The external data sets containing 80 patients were obtained from another hospital. Independent predictors of the 6-month unfavorable prognosis were analyzed using multivariate logistic regression. Furthermore, a nomogram prediction model was constructed using R software. After evaluation of the model, internal and external validations were performed to verify the efficiency of the model using the area under the receiver operating characteristic curves and the calibration plots.
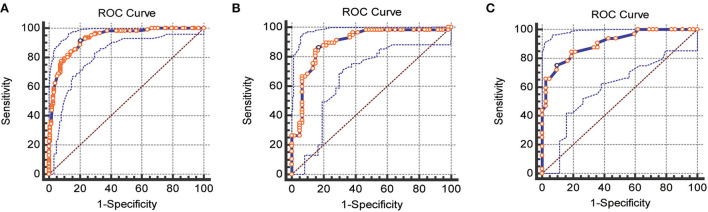
Results: In multivariate analysis, age(p = 0.001), Glasgow Score Scale (GCS) (p < 0.001), operative blood loss of >750 ml (p = 0.045), completely effaced basal cisterns (p < 0.001), intraoperative hypotension(p = 0.001), and activated partial thromboplastin time (APTT) of >36 (p = 0.012) were the early independent predictors for 6-month unfavorable prognosis in patients with TBI after primary DC. The AUC for the training, internal, and external validation cohorts was 0.93 (95%CI, 0.89-0.96, p < 0.0001), 0.89 (95%CI, 0.82-0.94, p < 0.0001), and 0.90 (95%CI, 0.84-0.97, p < 0.0001), respectively, which indicated that the prediction model had an excellent capability of discrimination. Calibration of the model was exhibited by the calibration plots, which showed an optimal concordance between the predicted 6-month unfavorable prognosis probability and actual probability in both training and validation cohorts.
Conclusion: This prediction model for a 6-month unfavorable prognosis in patients with TBI undergoing primary DC can evaluate the prognosis accurately and enhance the early identification of high-risk patients.
Keywords: decompressive craniectomy; nomogram; prognosis; traumatic brain injury; validation.
Copyright © 2022 Tang, Hu, Yang, Zou, Zhong, Huang, Wei and Jiang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
LinkOut - more resources
Full Text Sources