

Moderate and severe TBI in children and adolescents: The effects of age, sex, and injury severity on patient outcome 6 months after injury
- PMID: 35989939
- PMCID: PMC9382186
- DOI: 10.3389/fneur.2022.741717
Moderate and severe TBI in children and adolescents: The effects of age, sex, and injury severity on patient outcome 6 months after injury
Abstract
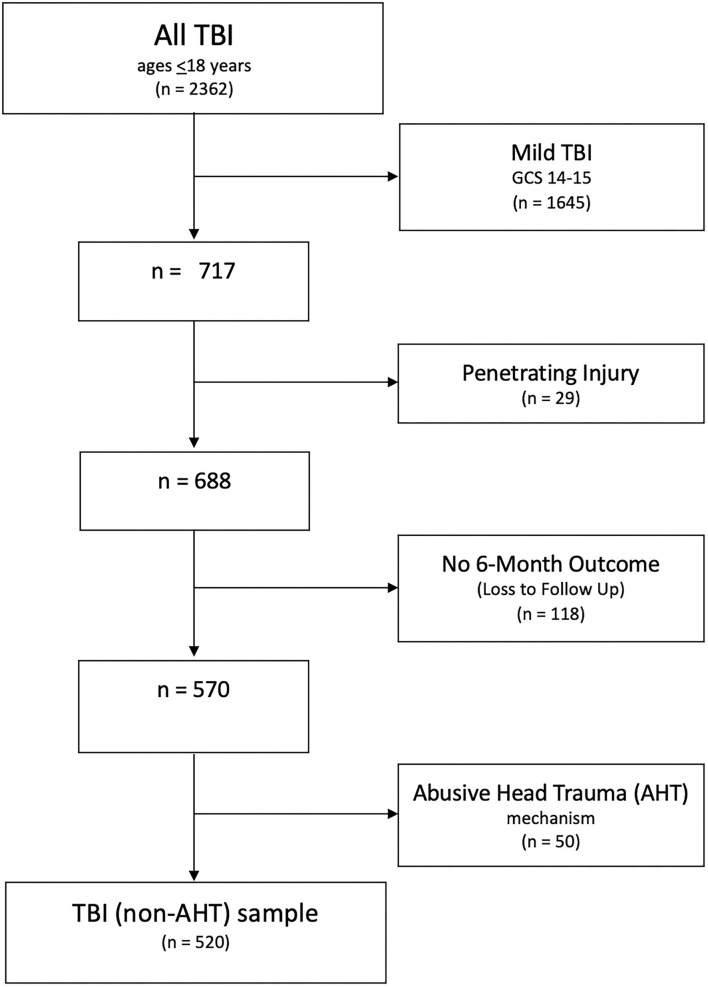
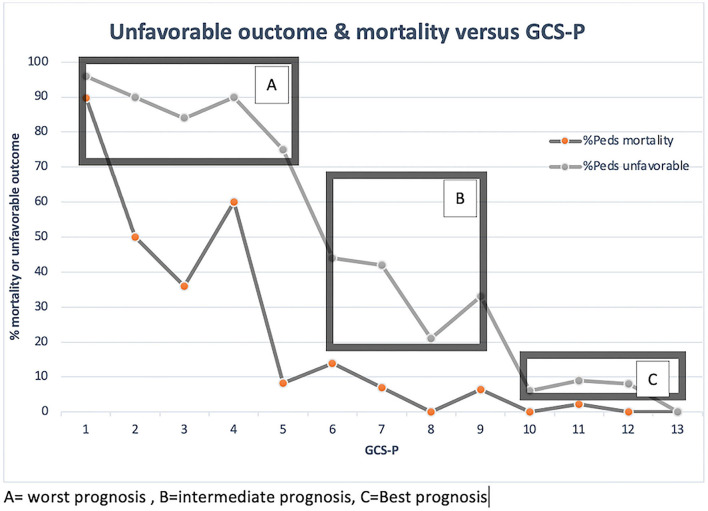
The interaction of age, sex, and outcomes of children with head injury remains incompletely understood and these factors need rigorous evaluation in prognostic models for pediatric head injury. We leveraged our large institutional pediatric TBI population to evaluate age and sex along with a series of predictive factors used in the acute care of injury to describe the response and outcome of children and adolescents with moderate to severe injury. We hypothesized that younger age at injury and male sex would be associated with adverse outcomes and that a novel GCS-based scale incorporating pupillary response (GCS-P) would have superior performance in predicting 6-month outcome. GCS and GCS-P along with established CT scan variables associated with neurologic outcomes were retrospectively reviewed in children (age birth to 18 years) with moderate or severe head injury. GOS-E was prospectively collected 6 months after injury; 570 patients were enrolled in the study, 520 with TBI and 50 with abusive head trauma, each analyzed separately. In the TBI cohort, the median age of patients was 8 years and 42.7% had a severe head injury. Multiple predictors of outcome were identified in univariate analysis; however, based on a multivariate analysis, the GCS was identified as most reliable, outperforming GCS-P, pupil score, and other clinical and CT scan predictors. After stratifying patients for severity of injury by GCS, no age- or sex-related effects were observed in our patient population, except for a trend toward worse outcomes in the neonatal group. Patients with abusive head trauma were more likely to have severe injury on presentation, increased mortality rate, and unfavorable outcome. Additionally, there was clear evidence that secondary injuries, including hypoxia, hypotension, and hypothermia were significantly associated with lower GCS and higher mortality in both AHT and TBI populations. Our findings support the use of GCS to guide clinical decision-making and prognostication in addition to emphasizing the need to stratify head injuries for severity when undertaking outcome studies. Finally, secondary injuries are a clear predictor of poor outcome and how we record and manage these events need to be considered moving forward.
Keywords: GCS-P; abusive head trauma; outcome; pediatric; prediction model; secondary injury; traumatic brain injury.
Copyright © 2022 Kennedy, Nuno, Gurkoff, Nosova and Zwienenberg.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Analysis of long-term (median 10.5 years) outcomes in children presenting with traumatic brain injury and an initial Glasgow Coma Scale score of 3 or 4.J Neurosurg Pediatr. 2015 Oct;16(4):410-9. doi: 10.3171/2015.3.PEDS14679. Epub 2015 Jul 3. J Neurosurg Pediatr. 2015. PMID: 26140392
-
Impact of Glasgow Coma Scale score and pupil parameters on mortality rate and outcome in pediatric and adult severe traumatic brain injury: a retrospective, multicenter cohort study.J Neurosurg. 2017 Mar;126(3):760-767. doi: 10.3171/2016.1.JNS152385. Epub 2016 Apr 1. J Neurosurg. 2017. PMID: 27035177
-
Simplifying the use of prognostic information in traumatic brain injury. Part 2: Graphical presentation of probabilities.J Neurosurg. 2018 Jun;128(6):1621-1634. doi: 10.3171/2017.12.JNS172782. Epub 2018 Apr 10. J Neurosurg. 2018. PMID: 29631517
-
Prognostic Significance of Magnetic Resonance Imaging in Detecting Diffuse Axonal Injuries: Analysis of Outcomes and Review of Literature.Neurol India. 2022 Nov-Dec;70(6):2371-2377. doi: 10.4103/0028-3886.364066. Neurol India. 2022. PMID: 36537418 Review.
-
Decompressive craniectomy for the treatment of high intracranial pressure in closed traumatic brain injury.Cochrane Database Syst Rev. 2019 Dec 31;12(12):CD003983. doi: 10.1002/14651858.CD003983.pub3. Cochrane Database Syst Rev. 2019. PMID: 31887790 Free PMC article.
Cited by
-
Traumatic brain injuries: a neuropsychological review.Front Behav Neurosci. 2024 Oct 8;18:1326115. doi: 10.3389/fnbeh.2024.1326115. eCollection 2024. Front Behav Neurosci. 2024. PMID: 39444788 Free PMC article. Review.
-
Neurological Pupillary Index (NPi) Measurement Using Pupillometry and Outcomes in Critically Ill Children.Cureus. 2023 Oct 4;15(10):e46480. doi: 10.7759/cureus.46480. eCollection 2023 Oct. Cureus. 2023. PMID: 37927706 Free PMC article.
-
Economic impact of reduced state trauma mortality on lifetime personal income and state tax revenue.Trauma Surg Acute Care Open. 2025 Jul 15;10(3):e001698. doi: 10.1136/tsaco-2024-001698. eCollection 2025. Trauma Surg Acute Care Open. 2025. PMID: 40673040 Free PMC article.
-
Acute Computer Tomography Findings in Pediatric Accidental Head Trauma-Review.Pediatric Health Med Ther. 2024 Jun 11;15:231-241. doi: 10.2147/PHMT.S461121. eCollection 2024. Pediatric Health Med Ther. 2024. PMID: 38882239 Free PMC article. Review.
-
Cognitive impairment in Chinese traumatic brain injury patients: from challenge to future perspectives.Front Neurosci. 2024 Mar 11;18:1361832. doi: 10.3389/fnins.2024.1361832. eCollection 2024. Front Neurosci. 2024. PMID: 38529265 Free PMC article. Review.
References
-
- CDC . Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations and Deaths 2002 - 2006. Atlanta, GA: CDC; (2010). p. 1–74.
-
- Ducrocq SC, Meyer PG, Orliaguet GA, Blanot S, Laurent-Vannier A, Renier D, et al. Epidemiology and early predictive factors of mortality and outcome in children with traumatic severe brain injury: experience of a French pediatric trauma center. Pediatr Crit Care Med. (2006) 7:461–7. 10.1097/01.PCC.0000235245.49129.27 - DOI - PubMed