

Light protection of parenteral nutrition, cholestasis, and other prematurity-related morbidities in premature infants
- PMID: 35989991
- PMCID: PMC9381878
- DOI: 10.3389/fped.2022.900068
Light protection of parenteral nutrition, cholestasis, and other prematurity-related morbidities in premature infants
Abstract
Introduction: Parenteral Nutrition (PN) can lead to intestinal failure associated liver disease (IFALD). There are no human studies to date studying specifically the benefits of light-protection on neonatal IFALD. Recently, the European Medicines Agency and the American Society for Parenteral and Enteral Nutrition (ASPEN) both recommended full light protection of PN to reduce the risk of adverse clinical outcomes.
Objective: The primary objective of this study was to evaluate the impact of light-protecting PN on the incidence of cholestasis and peak direct bilirubin levels in premature infants.
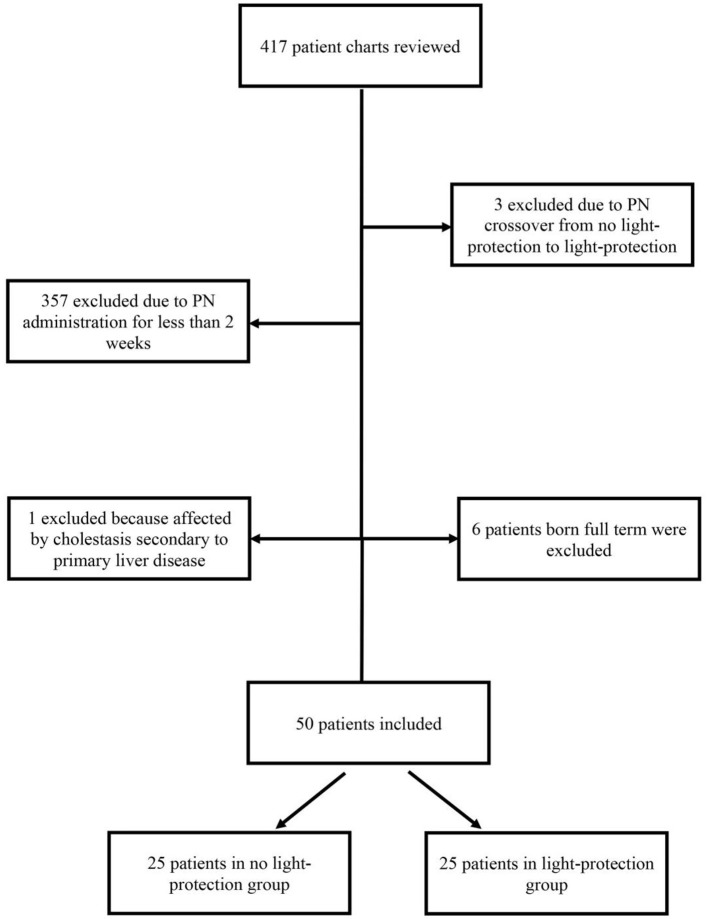
Study design: Retrospective chart review of preterm infants requiring PN for a minimum of 2 weeks with or without light-protection. After light protection of the PN solution, primary outcomes (including cholestasis and direct bilirubin levels) of both groups were compared. Secondary outcomes include evaluation of bronchopulmonary dysplasia (BPD), necrotizing enterocolitis (NEC), retinopathy of prematurity (ROP), sepsis and mortality.
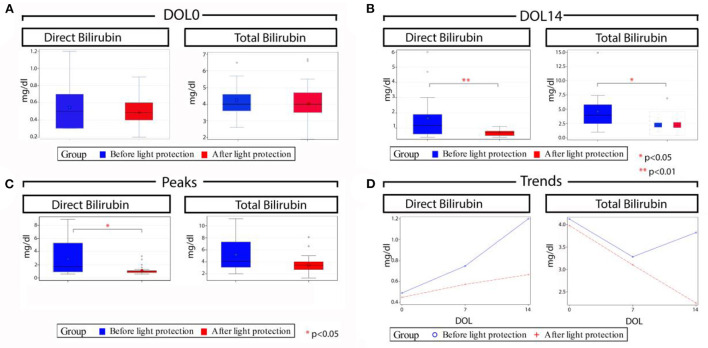
Results: A total of 50 preterm infants <37 weeks gestation were included, 25 infants in each group. There was a statistically significant decrease in the rate of cholestasis (12 vs. 3, p = 0.005), median peak direct bilirubin levels (1.7 vs. 0.9 mg/dL, p = 0.02) and total bilirubin levels (4.1 vs. 3.4, p = 0.05) in the light-protection group compared to no light-protection group. There was a decrease in the incidence of severe BPD (with an increase of mild BPD, resulting in the same overall BPD rate) in the light-protection compared to no light-protection group (7 vs. 15, p = 0.0223). There was no difference in NEC, ROP, sepsis or mortality.
Conclusion: Our study supports that the practice of light-protecting PN may reduce the incidence of IFALD in premature infants. Moreover, there was a trend toward decreased incidence of severe BPD in the light-protection group. Further light protection studies are needed to confirm these findings.
Keywords: bronchopulmonary dysplasia; cholestasis; direct hyperbilirubinemia; intestinal failure-associated liver disease; light protection; parenteral nutrition; premature infants.
Copyright © 2022 Clauss, Tack, Macchiarulo, Akerman, El-Chaar, Hanna and Tiozzo.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Lauriti G, Zani A, Aufieri R, Cananzi M, Chiesa PL, Eaton S, et al. . Incidence, prevention, and treatment of parenteral nutrition-associated cholestasis and intestinal failure-associated liver disease in infants and children: a systematic review. JPEN J Parenter Enteral Nutr. (2014) 38:70–85. 10.1177/0148607113496280 - DOI - PubMed
-
- Wales PW, Allen N, Worthington P, George D, Compher C, American Society for P et al. . ASPEN clinical guidelines: support of pediatric patients with intestinal failure at risk of parenteral nutrition-associated liver disease JPEN J Parenter Enteral Nutr. (2014) 38:538–57. 10.1177/0148607114527772 - DOI - PubMed
LinkOut - more resources
Full Text Sources