

Utility of umbilical cord blood 25-hydroxyvitamin D levels for predicting bronchopulmonary dysplasia in preterm infants with very low and extremely low birth weight
- PMID: 35989993
- PMCID: PMC9386287
- DOI: 10.3389/fped.2022.956952
Utility of umbilical cord blood 25-hydroxyvitamin D levels for predicting bronchopulmonary dysplasia in preterm infants with very low and extremely low birth weight
Abstract
Background and objective: There remains controversy regarding vitamin D deficiency and bronchopulmonary dysplasia (BPD) in very low birth weight (VLBW) and extremely low birth weight (ELBW) preterm infants. This study aimed to determine the prevalence of vitamin D deficiency assessed by umbilical cord blood 25-hydroxyvitamin D [25(OH)D] in preterm infants in northeast China and to evaluate the ability and optimal threshold of 25(OH)D for predicting BPD.
Methods: The clinical data of VLBW and ELBW preterm infants with known cord-blood 25(OH)D levels were analyzed retrospectively. Infants were divided into groups based on their cord-blood 25(OH)D levels and BPD diagnosis. Logistic regression was performed to assess the risk factors for BPD and a nomogram was established. Receiver operating characteristic (ROC) curve analysis was used to evaluate the optimal threshold of cord-blood 25(OH)D concentration for predicting BPD.
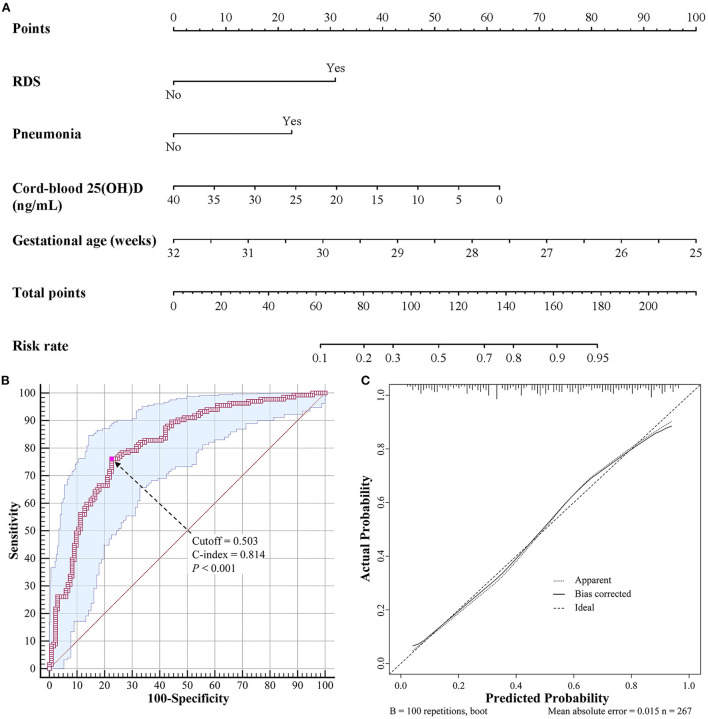
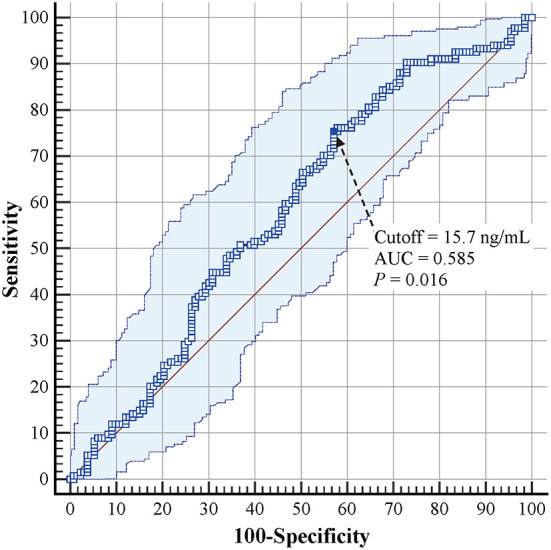
Results: A total of 267 preterm infants were included, of which 225 (84.3%) exhibited vitamin D deficiency and 134 (50.2%) were diagnosed with BPD. The incidence of BPD was lower in the group with a 25(OH)D level of >20 ng/ml than in the other groups (P = 0.024). Infants with BPD had lower cord-blood 25(OH)D levels than those without BPD (11.6 vs. 13.6 ng/ml, P = 0.016). The multivariate logistic regression model revealed that 25(OH)D levels (odds ratio [OR] = 0.933, 95% confidence interval [95% CI]: 0.891-0.977), gestational age (OR = 0.561, 95% CI: 0.425-0.740), respiratory distress syndrome (OR = 2.989, 95% CI: 1.455-6.142), and pneumonia (OR = 2.546, 95% CI: 1.398-4.639) were independent risk factors for BPD. A predictive nomogram containing these four risk factors was established, which had a C-index of 0.814. ROC curve analysis revealed that the optimal cutoff value of 25(OH)D for predicting BPD was 15.7 ng/ml (area under the curve = 0.585, 95% CI: 0.523-0.645, P = 0.016), with a sensitivity of 75.4% and a specificity of 42.9%.
Conclusions: A cord-blood 25(OH)D level of <15.7 ng/ml was predictively valuable for the development of BPD. The nomogram established in this study can help pediatricians predict the risk of BPD more effectively and easily.
Keywords: 25-hydroxyvitamin D; bronchopulmonary dysplasia; extremely low birth weight infants; preterm infants; very low birth weight infants.
Copyright © 2022 Yu, Fu and Feng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources