

Imagining a Personalized Scenario Selectively Increases Perceived Risk of Viral Transmission for Older Adults
- PMID: 35990532
- PMCID: PMC9387905
- DOI: 10.1038/s43587-021-00095-7
Imagining a Personalized Scenario Selectively Increases Perceived Risk of Viral Transmission for Older Adults
Abstract
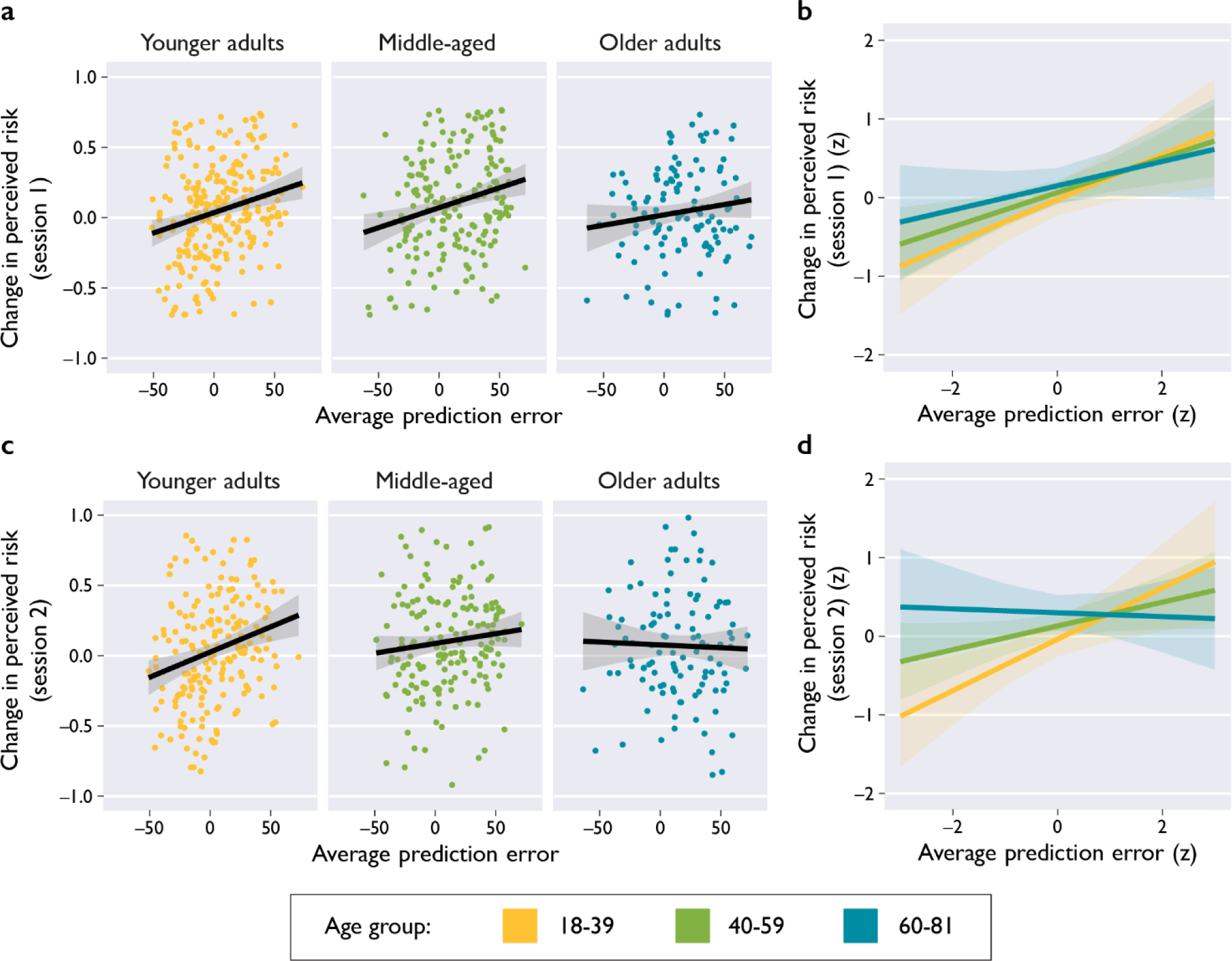
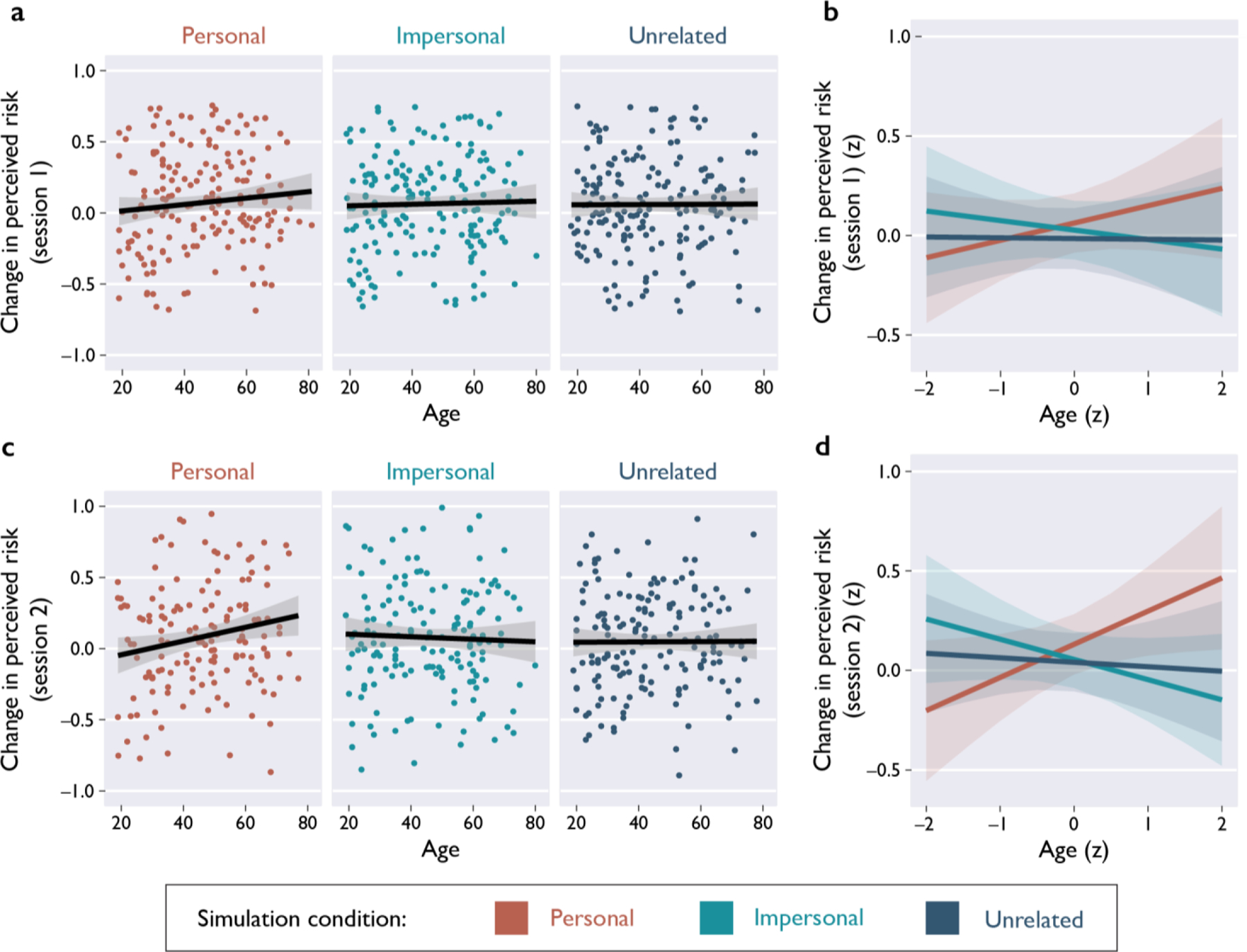
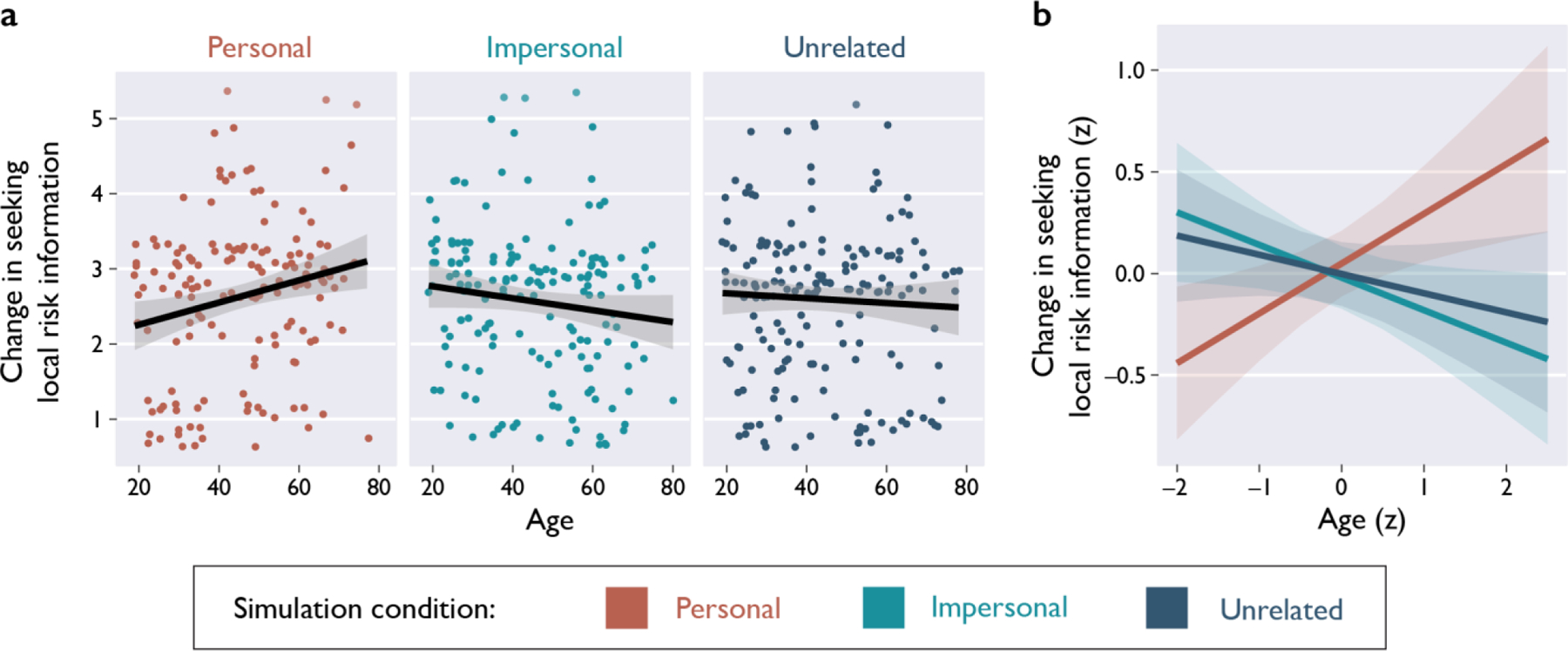
The COVID-19 pandemic has created a serious and prolonged public-health emergency. Older adults have been at substantially greater risk of hospitalization, ICU admission, and death due to COVID-19; as of February 2021, over 81% of COVID-19-related deaths in the U.S. occurred for people over the age of 651,2. Converging evidence from around the world suggests that age is the greatest risk factor for severe COVID-19 illness and for the experience of adverse health outcomes3,4. Therefore, effectively communicating health-related risk information requires tailoring interventions to older adults' needs5. Using a novel informational intervention with a nationally-representative sample of 546 U.S. residents, we found that older adults reported increased perceived risk of COVID-19 transmission after imagining a personalized scenario with social consequences. Although older adults tended to forget numerical information over time, the personalized simulations elicited increases in perceived risk that persisted over a 1-3 week delay. Overall, our results bear broad implications for communicating information about health risks to older adults, and they suggest new strategies to combat annual influenza outbreaks.
Keywords: COVID-19; aging; cognition; decision-making; episodic simulation; memory; risk perception; socioemotional selectivity.
Conflict of interest statement
Competing Interests Statement: The authors have no competing interests to report.
Figures
Comment in
-
Risks, real and imagined.Nat Aging. 2021 Aug;1(8):628-630. doi: 10.1038/s43587-021-00097-5. Nat Aging. 2021. PMID: 37117766 No abstract available.
Similar articles
-
Pairing facts with imagined consequences improves pandemic-related risk perception.Proc Natl Acad Sci U S A. 2021 Aug 10;118(32):e2100970118. doi: 10.1073/pnas.2100970118. Proc Natl Acad Sci U S A. 2021. PMID: 34341120 Free PMC article.
-
Contrasting Objective and Perceived Risk: Predicting COVID-19 Health Behaviors in a Nationally Representative U.S. Sample.Ann Behav Med. 2024 Mar 12;58(4):242-252. doi: 10.1093/abm/kaad055. Ann Behav Med. 2024. PMID: 38413045
-
How Has the Nationwide Public Health Emergency of the COVID-19 Pandemic Affected Older Chinese Adults' Health Literacy, Health Behaviors and Practices, and Social Connectedness? Qualitative Evidence From Urban China.Front Public Health. 2022 Mar 10;9:774675. doi: 10.3389/fpubh.2021.774675. eCollection 2021. Front Public Health. 2022. PMID: 35356089 Free PMC article.
-
Identifying models of care to improve outcomes for older people with urgent care needs: a mixed methods approach to develop a system dynamics model.Health Soc Care Deliv Res. 2023 Sep;11(14):1-183. doi: 10.3310/NLCT5104. Health Soc Care Deliv Res. 2023. PMID: 37830206 Review.
-
Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: a rapid review.Cochrane Database Syst Rev. 2020 May 14;5(5):CD013600. doi: 10.1002/14651858.CD013600. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Jul 10;7:CD013600. doi: 10.1002/14651858.CD013600.pub2. PMID: 32406927 Free PMC article. Updated.
Cited by
-
Social divisions and risk perception drive divergent epidemics and large later waves.Evol Hum Sci. 2023 Feb 23;5:e8. doi: 10.1017/ehs.2023.2. eCollection 2023. Evol Hum Sci. 2023. PMID: 37587926 Free PMC article.
-
Clinician and patient perspectives on screening mammography among women age 75 and older: A pilot study of a novel decision aid.PEC Innov. 2023 Dec;2:100132. doi: 10.1016/j.pecinn.2023.100132. Epub 2023 Jan 31. PEC Innov. 2023. PMID: 37124453 Free PMC article.
-
Episodic Future Thinking and COVID-19 Vaccination Intent in Trauma-Exposed Military Veterans: A Pilot Study.Behav Ther (N Y N Y). 2022;45(3):96-99. Behav Ther (N Y N Y). 2022. PMID: 38584963 Free PMC article. No abstract available.
-
Scenario-Based Messages on Social Media Motivate COVID-19 Information Seeking.J Appl Res Mem Cogn. 2024 Mar;13(1):124-135. doi: 10.1037/mac0000114. Epub 2023 Apr 27. J Appl Res Mem Cogn. 2024. PMID: 38655203 Free PMC article.
-
Episodic simulation of helping behavior in younger and older adults during the COVID-19 pandemic.J Appl Res Mem Cogn. 2023 Sep;12(3):443-456. doi: 10.1037/mac0000073. Epub 2022 Oct 20. J Appl Res Mem Cogn. 2023. PMID: 37873548 Free PMC article.
References
-
- CDC. COVID Data Tracker. Centers for Disease Control and Prevention https://covid.cdc.gov/covid-data-tracker (2021).
-
- Stratton C, Andersen L, Proulx L & Sirotich E When apathy is deadlier than COVID-19. Nat. Aging 1, 144–145 (2021). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
