

Pre-procedural planning of coronary revascularization by cardiac computed tomography: An expert consensus document of the Society of Cardiovascular Computed Tomography
- PMID: 35994043
- PMCID: PMC9743242
- DOI: 10.4244/EIJ-E-22-00036
Pre-procedural planning of coronary revascularization by cardiac computed tomography: An expert consensus document of the Society of Cardiovascular Computed Tomography
Abstract
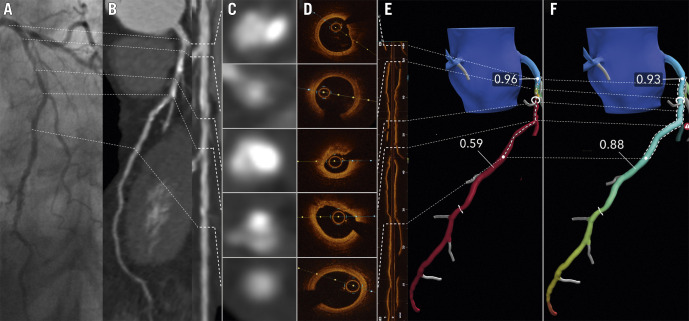
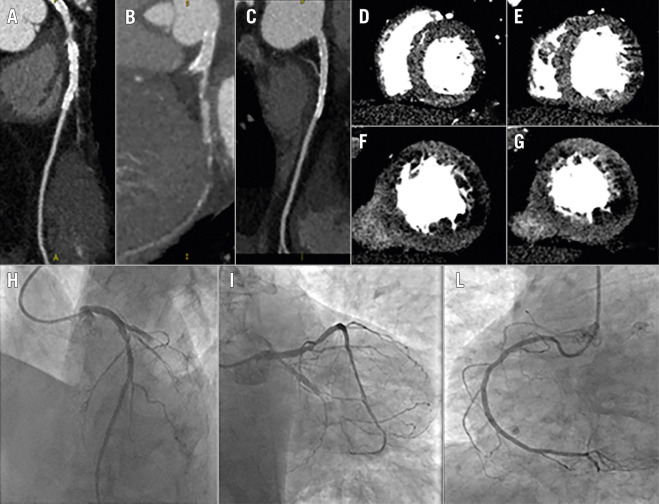
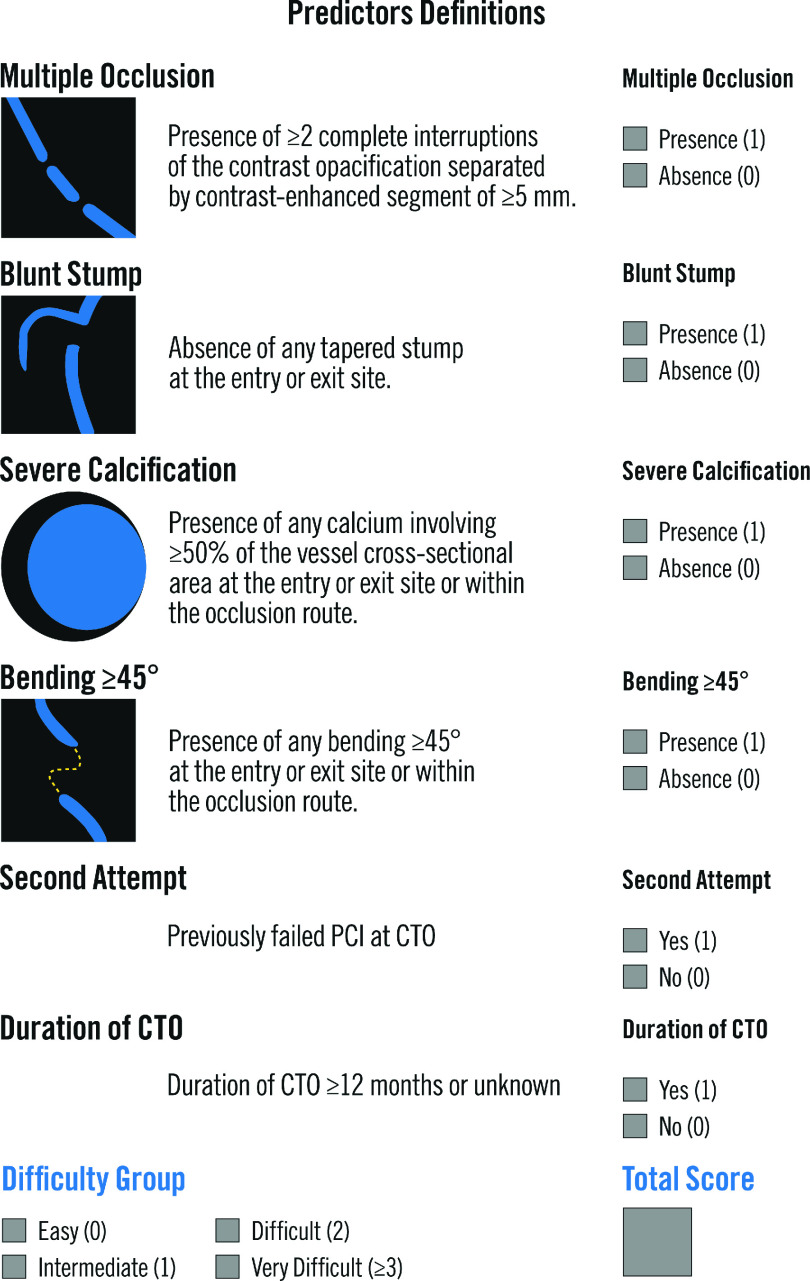
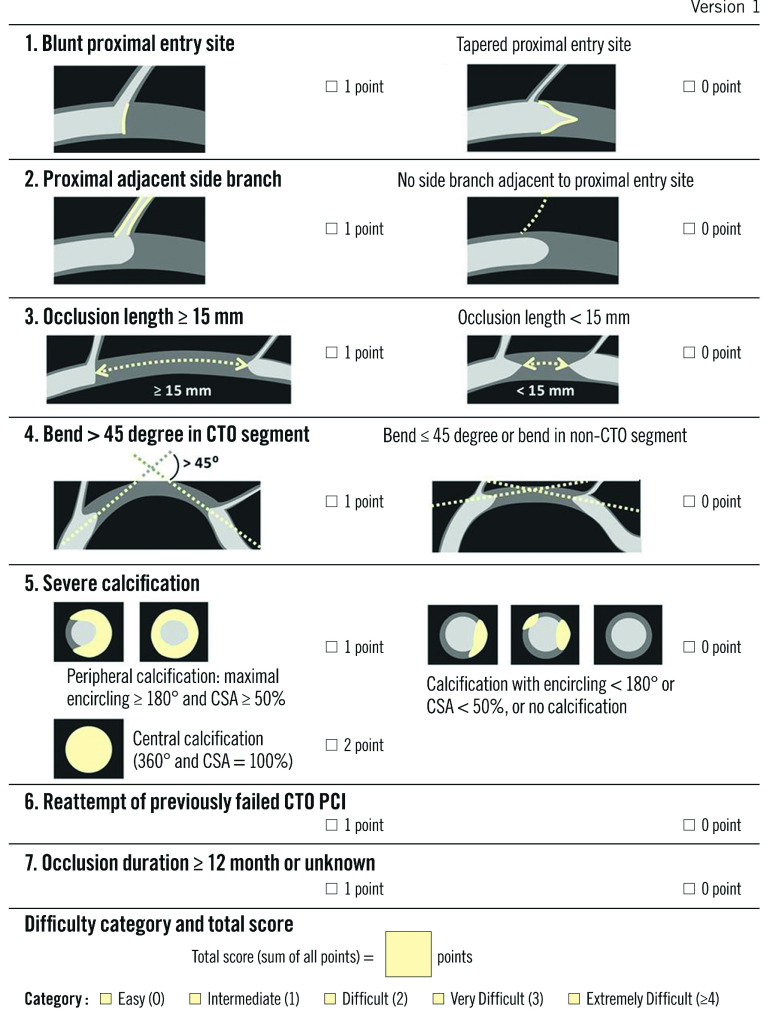
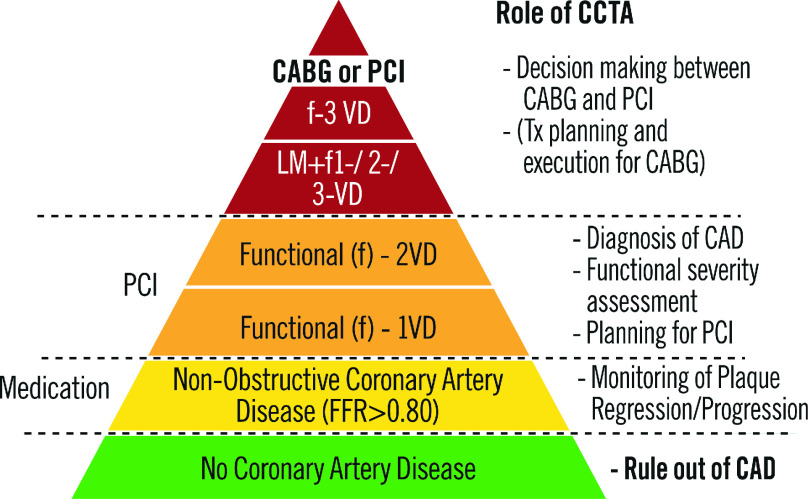
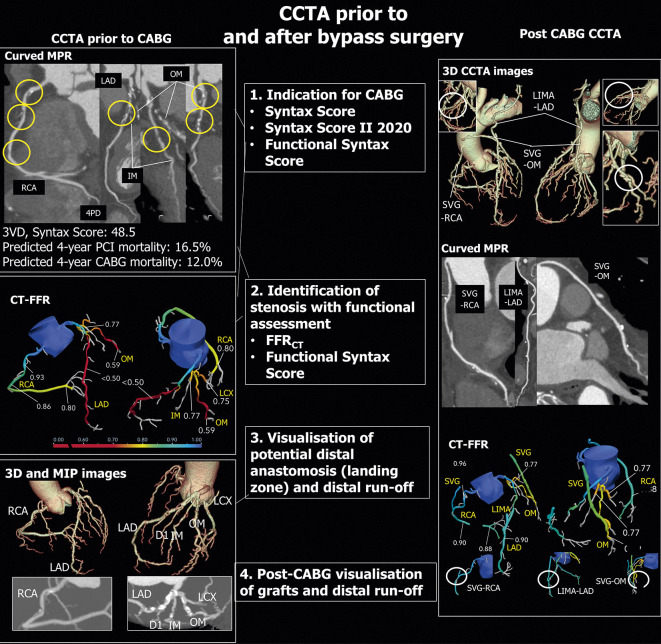
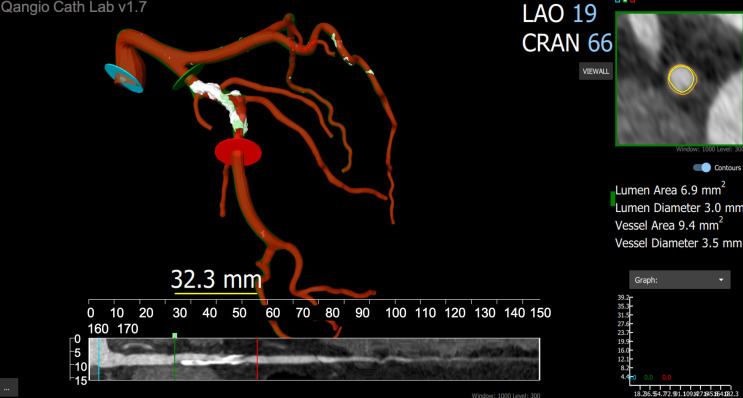
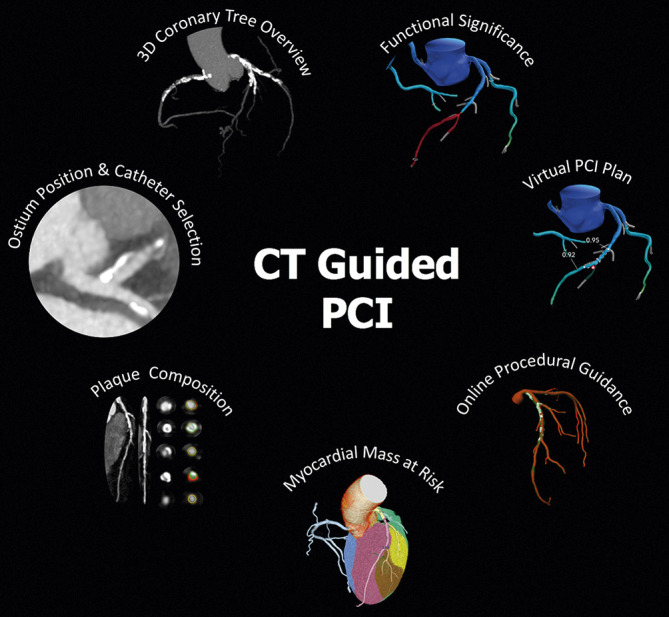
Coronary CT angiography (CCTA) demonstrated high diagnostic accuracy for detecting coronary artery disease (CAD) and a key role in the management of patients with low-to-intermediate pretest likelihood of CAD. However, the clinical information provided by this noninvasive method is still regarded insufficient in patients with diffuse and complex CAD and for planning percutaneous coronary intervention (PCI) and surgical revascularization procedures. On the other hand, technology advancements have recently shown to improve CCTA diagnostic accuracy in patients with diffuse and calcific stenoses. Moreover, stress CT myocardial perfusion imaging (CT-MPI) and fractional flow reserve derived from CCTA (CT-FFR) have been introduced in clinical practice as new tools for evaluating the functional relevance of coronary stenoses, with the possibility to overcome the main CCTA drawback, i.e. anatomical assessment only. The potential value of CCTA to plan and guide interventional procedures lies in the wide range of information it can provide: a) detailed evaluation of plaque extension, volume and composition; b) prediction of procedural success of CTO PCI using scores derived from CCTA; c) identification of coronary lesions requiring additional techniques (e.g., atherectomy and lithotripsy) to improve stent implantation success by assessing calcium score and calcific plaque distribution; d) assessment of CCTA-derived Syntax Score and Syntax Score II, which allows to select the mode of revascularization (PCI or CABG) in patients with complex and multivessel CAD. The aim of this Consensus Document is to review and discuss the available data supporting the role of CCTA, CT-FFR and stress CT-MPI in the preprocedural and possibly intraprocedural planning and guidance of myocardial revascularization interventions.
Figures
References
-
- Stein PD, Yaekoub AY, Matta F, Sostman HD. 64-slice CT for diagnosis of coronary artery disease: a systematic review. Am J Med. 2008;121(8):715–25. - PubMed
-
- Schroeder S, Achenbach S, Bengel F, et al. Working group nuclear cardiology and cardiac CT; European Society of cardiology; European Council of nuclear cardiology. Cardiac computed tomography: indications, applications, limitations, and training requirements: report of a writing group deployed by the working group nuclear cardiology and cardiac CT of the European Society of cardiology and the European Council of nuclear cardiology. Eur Heart J. 2008;29(4):531–56. - PubMed
-
- Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 2008;52(21):1724–32. - PubMed
-
- Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008;52(25):2135–44. - PubMed
-
- Marano R, De Cobelli F, Floriani I, et al, NIMISCAD Study Group. Italian multicenter, prospective study to evaluate the negative predictive value of 16- and 64-slice MDCT imaging in patients scheduled for coronary angiography (NIMISCAD-Non Invasive Multicenter Italian Study for Coronary Artery Disease). Eur Radiol. 2009;19(5):1114–23. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous