

Clinical Features and Burden of Postacute Sequelae of SARS-CoV-2 Infection in Children and Adolescents
- PMID: 35994282
- PMCID: PMC9396470
- DOI: 10.1001/jamapediatrics.2022.2800
Clinical Features and Burden of Postacute Sequelae of SARS-CoV-2 Infection in Children and Adolescents
Abstract
Importance: The postacute sequelae of SARS-CoV-2 infection (PASC) has emerged as a long-term complication in adults, but current understanding of the clinical presentation of PASC in children is limited.
Objective: To identify diagnosed symptoms, diagnosed health conditions, and medications associated with PASC in children.
Design, setting and participants: This retrospective cohort study used electronic health records from 9 US children's hospitals for individuals younger than 21 years who underwent antigen or reverse transcriptase-polymerase chain reaction (RT-PCR) testing for SARS-CoV-2 between March 1, 2020, and October 31, 2021, and had at least 1 encounter in the 3 years before testing.
Exposures: SARS-CoV-2 positivity by viral test (antigen or RT-PCR).
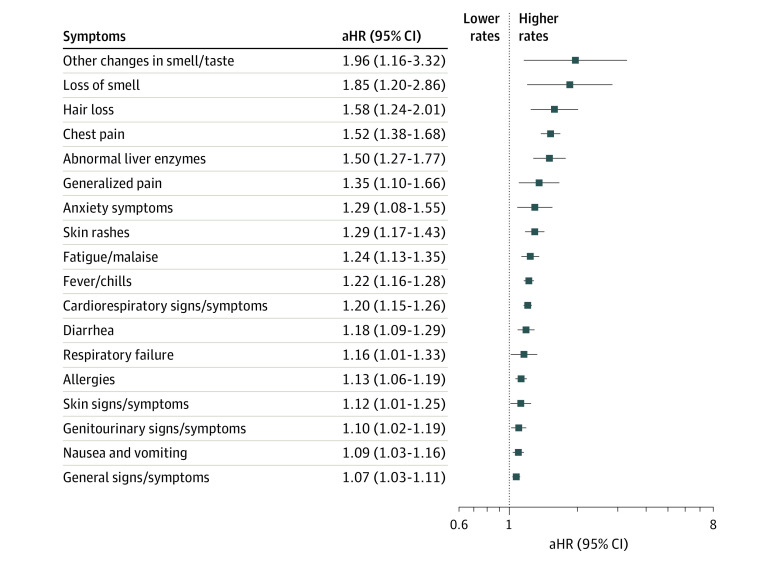
Main outcomes and measures: Syndromic (symptoms), systemic (conditions), and medication PASC features were identified in the 28 to 179 days following the initial test date. Adjusted hazard ratios (aHRs) were obtained for 151 clinically predicted PASC features by contrasting viral test-positive groups with viral test-negative groups using proportional hazards models, adjusting for site, age, sex, testing location, race and ethnicity, and time period of cohort entrance. The incidence proportion for any syndromic, systemic, or medication PASC feature was estimated in the 2 groups to obtain a burden of PASC estimate.
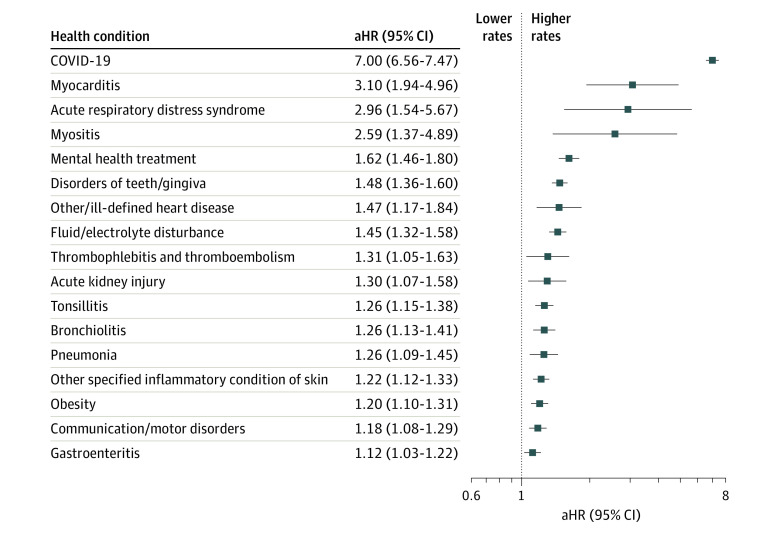
Results: Among 659 286 children in the study sample, 348 091 (52.8%) were male, and the mean (SD) age was 8.1 (5.7) years. A total of 59 893 (9.1%) tested positive by viral test for SARS-CoV-2, and 599 393 (90.9%) tested negative. Most were tested in outpatient testing facility settings (322 813 [50.3%]) or office settings (162 138 [24.6%]). The most common syndromic, systemic, and medication features were loss of taste or smell (aHR, 1.96; 95% CI, 1.16-3.32), myocarditis (aHR, 3.10; 95% CI, 1.94-4.96), and cough and cold preparations (aHR, 1.52; 95% CI, 1.18-1.96), respectively. The incidence of at least 1 systemic, syndromic, or medication feature of PASC was 41.9% (95% CI, 41.4-42.4) among viral test-positive children vs 38.2% (95% CI, 38.1-38.4) among viral test-negative children, with an incidence proportion difference of 3.7% (95% CI, 3.2-4.2). A higher strength of association for PASC was identified in those cared for in the intensive care unit during the acute illness phase, children younger than 5 years, and individuals with complex chronic conditions.
Conclusions and relevance: In this large-scale, exploratory study, the burden of pediatric PASC that presented to health systems was low. Myocarditis was the most commonly diagnosed PASC-associated condition. Acute illness severity, young age, and comorbid complex chronic disease increased the risk of PASC.
Conflict of interest statement
Figures
Update of
-
Clinical features and burden of post-acute sequelae of SARS-CoV-2 infection in children and adolescents: an exploratory EHR-based cohort study from the RECOVER program.medRxiv [Preprint]. 2022 May 25:2022.05.24.22275544. doi: 10.1101/2022.05.24.22275544. medRxiv. 2022. Update in: JAMA Pediatr. 2022 Oct 1;176(10):1000-1009. doi: 10.1001/jamapediatrics.2022.2800. PMID: 35665016 Free PMC article. Updated. Preprint.
Comment in
-
Further evidence from a large US electronic health record-based study that some children and adolescents can develop postacute sequelae of SARS-CoV-2 infection.Evid Based Nurs. 2023 Jul;26(3):97. doi: 10.1136/ebnurs-2022-103632. Epub 2023 Jan 4. Evid Based Nurs. 2023. PMID: 36599668 No abstract available.
References
-
- RECOVER . Homepage. Accessed April 12, 2022, https://recovercovid.org/
-
- US Centers for Disease Control and Prevention . Interim guidance on evaluating and caring for patients with post-COVID conditions. Accessed December 22, 2021. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-i...
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
