

Magnetic Resonance Imaging for Spine Emergencies
- PMID: 35995469
- PMCID: PMC9926664
- DOI: 10.1016/j.mric.2022.04.004
Magnetic Resonance Imaging for Spine Emergencies
Abstract
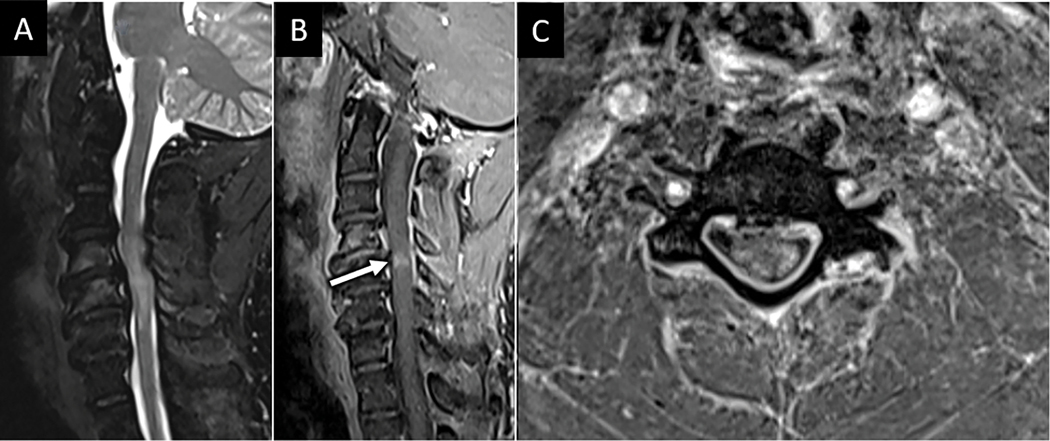
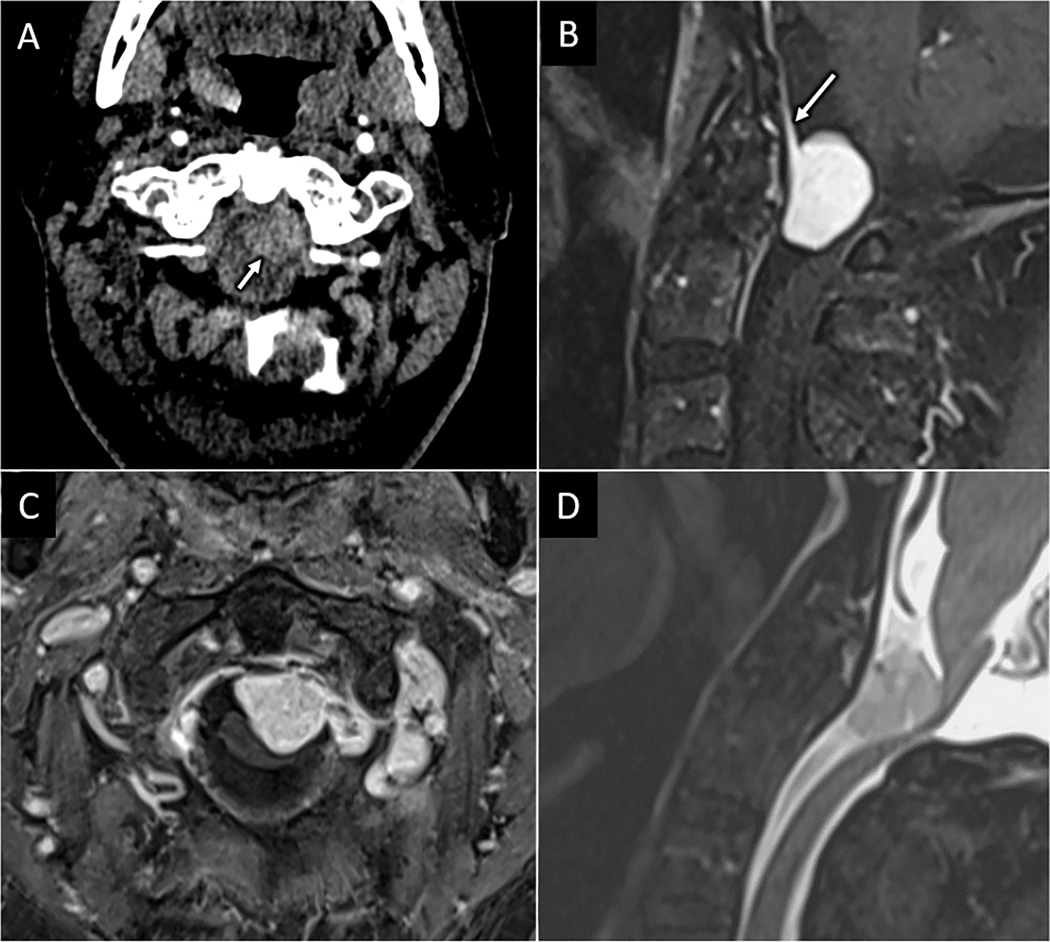
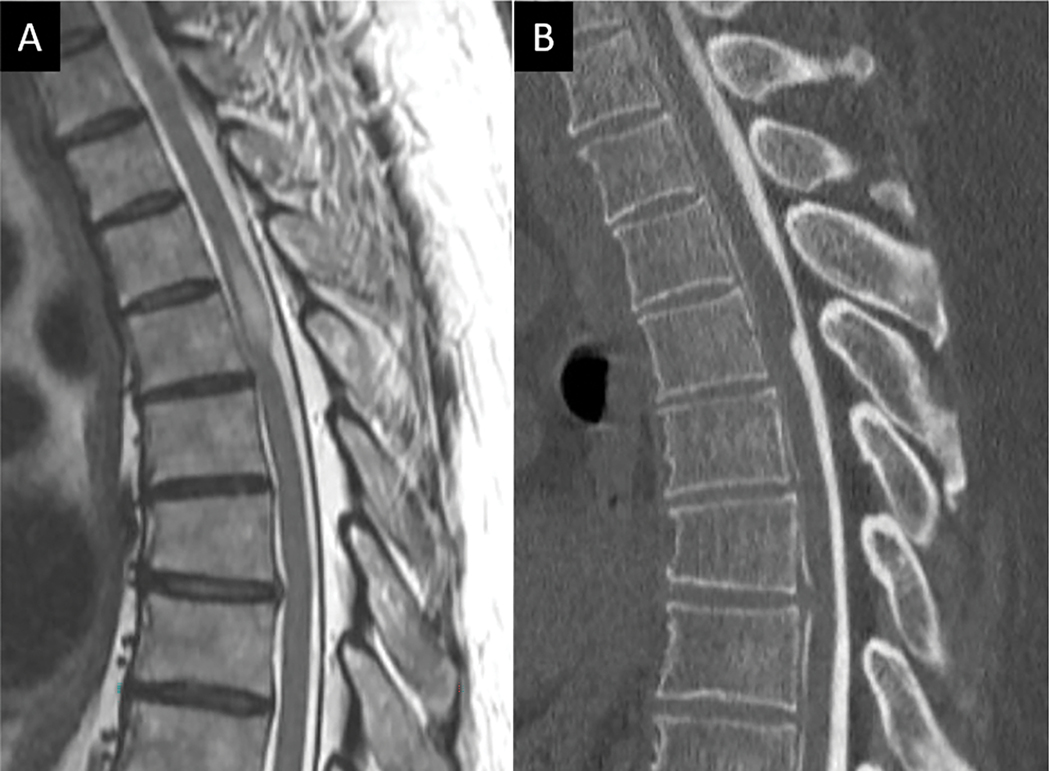
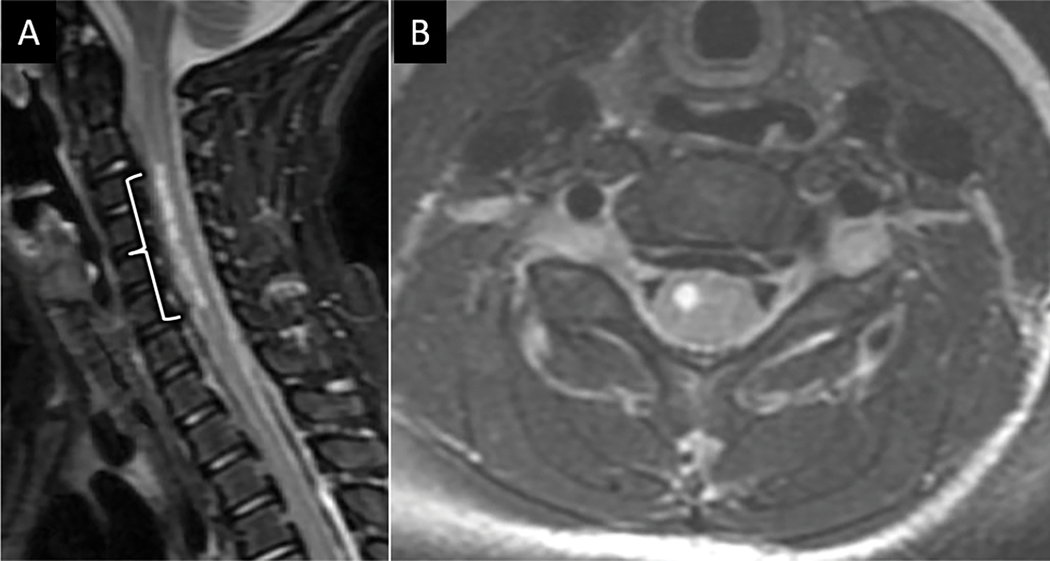
This article is devoted to the MR imaging evaluation of spine emergencies, defined as spinal pathologic conditions that pose an immediate risk of significant morbidity or mortality to the patient if not diagnosed and treated in a timely manner. MR imaging plays a central role in the timely diagnosis of spine emergencies. A summary of MR imaging indications and MR imaging protocols tailored for a variety of spinal emergencies will be presented followed by a review of key imaging findings for the most-encountered emergent spine pathologic conditions. Pathologic conditions will be broadly grouped into traumatic and atraumatic pathologic conditions. For traumatic injuries, a practical and algorithmic diagnostic approach based on the AO Spine injury classification system will be presented focused on subaxial spine trauma. Atraumatic spinal emergencies will be dichotomized into compressive and noncompressive subtypes. The location of external compressive disease with respect to the thecal sac is fundamental to establishing a differential diagnosis for compressive emergencies, whereas specific patterns of spinal cord involvement on MR imaging will guide the discussion of inflammatory and noninflammatory causes of noncompressive myelopathy.
Keywords: MR imaging; Myelitis; Myelopathy; Spinal cord; Spinal cord injury.
Copyright © 2022 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure The authors have nothing to disclose
Figures
References
-
- Arce D, Sass P, Abul-Khoudoud H. Recognizing spinal cord emergencies. Am Fam Physician. Aug 15 2001;64(4):631–8. - PubMed
