

Out-of-hospital cardiac arrest and in-hospital mortality among COVID-19 patients: A population-based retrospective cohort study
- PMID: 35995669
- PMCID: PMC9365707
- DOI: 10.1016/j.jmii.2022.07.009
Out-of-hospital cardiac arrest and in-hospital mortality among COVID-19 patients: A population-based retrospective cohort study
Abstract
Background/purpose: Predictors for out-of-hospital cardiac arrest (OHCA) in COVID-19 patients remain unclear. We identified the predictors for OHCA and in-hospital mortality among such patients in community isolation centers.
Methods: From May 15 to June 20, 2021, this cohort study recruited 2555 laboratory-confirmed COVID-19 patients admitted to isolation centers in Taiwan. All patients were followed up until death, discharge from the isolation center or hospital, or July 16, 2021. OHCA was defined as cardiac arrest confirmed by the absence of circulation signs and occurring outside the hospital. Multinomial logistic regressions were used to determine factors associated with OHCA and in-hospital mortality.
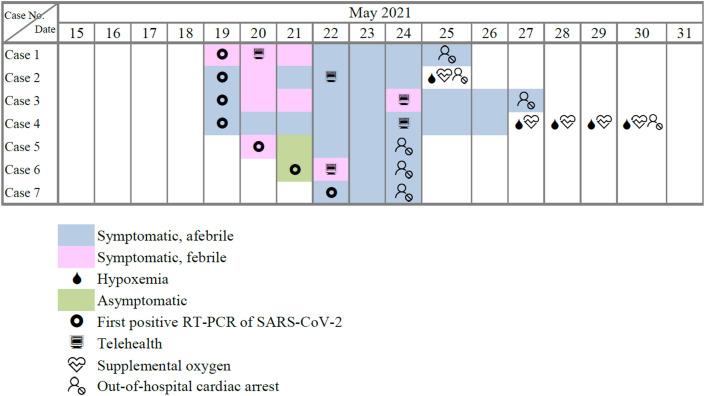
Results: Of the 37 deceased patients, 7 (18.9%) had OHCA and 30 (81.1%) showed in-hospital mortality. The mean (SD) time to OHCA was 6.6 (3.3) days from the symptom onset. After adjusting for demographics and comorbidities, independent predictors for OHCA included age ≥65 years (adjusted odds ratio [AOR]: 13.24, 95% confidence interval [CI]: 1.85-94.82), fever on admission to the isolation center (AOR: 12.53, 95% CI: 1.68-93.34), and hypoxemia (an oxygen saturation level below 95% on room air) (AOR: 26.54, 95% CI: 3.18-221.73). Predictors for in-hospital mortality included age ≥65 years (AOR: 10.28, 95% CI: 2.95-35.90), fever on admission to the isolation centers (AOR: 7.27, 95% CI: 1.90-27.83), and hypoxemia (AOR: 29.87, 95% CI: 10.17-87.76).
Conclusions: Time to OHCA occurrence is rapid in COVID-19 patients. Close monitoring of patients' vital signs and disease severity during isolation is important, particularly for those with older age, fever, and hypoxemia.
Keywords: COVID-19; Hypoxemia; Mortality; Out-of-hospital cardiac arrest; SARS-CoV-2.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
Declaration of competing interest No conflict of interest exists for the author.
Figures
Similar articles
-
Impact of Transport Time and Cardiac Arrest Centers on the Neurological Outcome After Out-of-Hospital Cardiac Arrest: A Retrospective Cohort Study.J Am Heart Assoc. 2020 Jun 2;9(11):e015544. doi: 10.1161/JAHA.119.015544. Epub 2020 May 27. J Am Heart Assoc. 2020. PMID: 32458720 Free PMC article.
-
Outcomes for Out-of-Hospital Cardiac Arrest in the United States During the Coronavirus Disease 2019 Pandemic.JAMA Cardiol. 2021 Mar 1;6(3):296-303. doi: 10.1001/jamacardio.2020.6210. JAMA Cardiol. 2021. PMID: 33188678 Free PMC article.
-
[Investigation of out-of-hospital cardiac arrest in Zhengzhou City and the risk factors of prognosis of cardiopulmonary resuscitation: case analysis for 2016-2018].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Apr;31(4):439-443. doi: 10.3760/cma.j.issn.2095-4352.2019.04.013. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31109417 Chinese.
-
Epidemiology and Outcome of Out-of-Hospital Cardiac Arrests during the COVID-19 Pandemic in South Korea: A Systematic Review and Meta-Analyses.Yonsei Med J. 2022 Dec;63(12):1121-1129. doi: 10.3349/ymj.2022.0339. Yonsei Med J. 2022. PMID: 36444548 Free PMC article.
-
Community first responders for out-of-hospital cardiac arrest in adults and children.Cochrane Database Syst Rev. 2019 Jul 19;7(7):CD012764. doi: 10.1002/14651858.CD012764.pub2. Cochrane Database Syst Rev. 2019. PMID: 31323120 Free PMC article.
Cited by
-
Coronavirus disease 2019 rebounds following nirmatrelvir/ritonavir treatment.J Med Virol. 2023 Feb;95(2):e28430. doi: 10.1002/jmv.28430. J Med Virol. 2023. PMID: 36571273 Free PMC article. Review.
References
-
- World health organization: coronavirus disease (COVID-19) pandemic. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/
-
- Taiwan Centers for Disease Control and Prevention [Surveillance of COVID-19] https://www.cdc.gov.tw/En
-
- COVID-19 vaccination in taiwan. https://covid-19.nchc.org.tw/dt_002-csse_covid_19_daily_reports_vaccine_...
-
- Taiwan Centers for Disease Control and Prevention [Clinical management of COVID-19 patients] https://www.cdc.gov.tw/Category/Page/xCSwc5oznwcqunujPc-qmQ
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
