

Antiviral and clinical activity of bamlanivimab in a randomized trial of non-hospitalized adults with COVID-19
- PMID: 35995785
- PMCID: PMC9395368
- DOI: 10.1038/s41467-022-32551-2
Antiviral and clinical activity of bamlanivimab in a randomized trial of non-hospitalized adults with COVID-19
Erratum in
-
Publisher Correction: Antiviral and clinical activity of bamlanivimab in a randomized trial of non-hospitalized adults with COVID-19.Nat Commun. 2023 Jan 19;14(1):333. doi: 10.1038/s41467-023-35835-3. Nat Commun. 2023. PMID: 36658128 Free PMC article. No abstract available.
Abstract
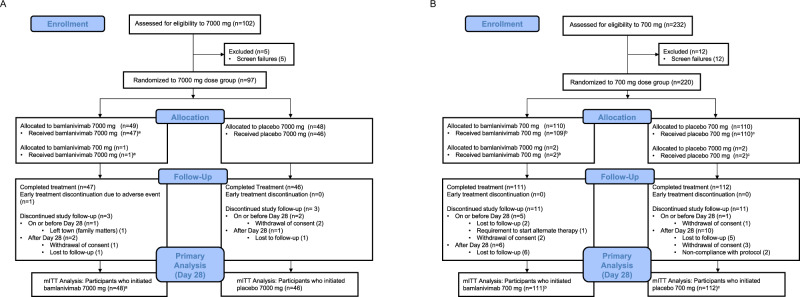
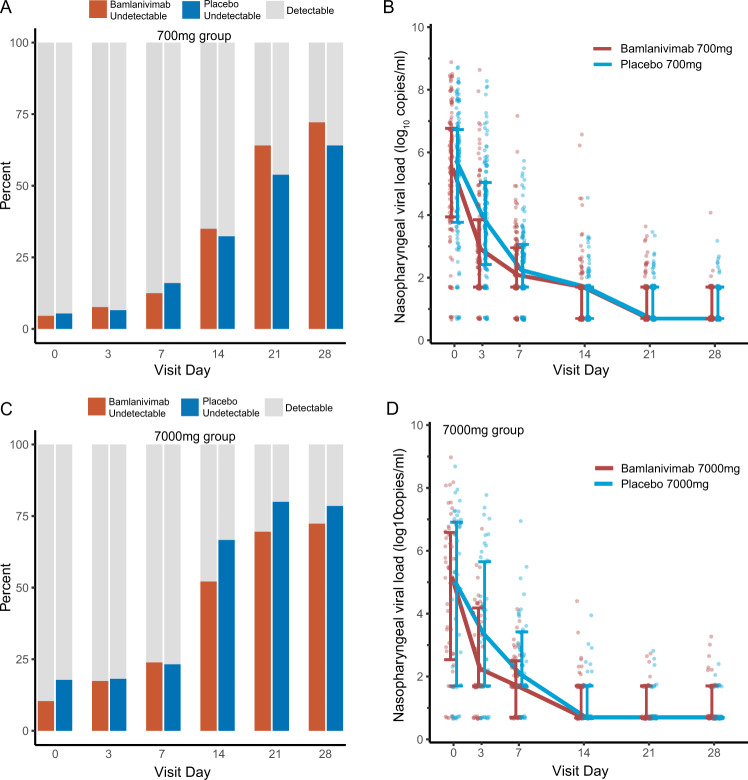
Anti-SARS-CoV-2 monoclonal antibodies are mainstay COVID-19 therapeutics. Safety, antiviral, and clinical efficacy of bamlanivimab were evaluated in the randomized controlled trial ACTIV-2/A5401. Non-hospitalized adults were randomized 1:1 within 10 days of COVID-19 symptoms to bamlanivimab or blinded-placebo in two dose-cohorts (7000 mg, n = 94; 700 mg, n = 223). No differences in bamlanivimab vs placebo were observed in the primary outcomes: proportion with undetectable nasopharyngeal SARS-CoV-2 RNA at days 3, 7, 14, 21, and 28 (risk ratio = 0.82-1.05 for 7000 mg [p(overall) = 0.88] and 0.81-1.21 for 700 mg [p(overall) = 0.49]), time to symptom improvement (median 21 vs 18.5 days [p = 0.97], 7000 mg; 24 vs 20.5 days [p = 0.08], 700 mg), or grade 3+ adverse events. However, bamlanivimab was associated with lower day 3 nasopharyngeal viral levels and faster reductions in inflammatory markers and viral decay by modeling. This study provides evidence of faster reductions in nasopharyngeal SARS-CoV-2 RNA levels but not shorter symptom durations in non-hospitalized adults with early variants of SARS-CoV-2.
© 2022. The Author(s).
Conflict of interest statement
K.W.C. has received research funding to the institution from Merck Sharp & Dohme and is a consultant for Pardes Biosciences. E.S.D. receives consulting fees from Gilead Sciences, Merck, and GSK/ViiV and research support through the institution from Gilead Sciences and GSK/ViiV. D.A.W. has received funding to the institution to support research and honoraria for advisory boards and consulting from Gilead Sciences. J.Z.L. has consulted for Abbvie. C.M. has received research funding to the institution from E.L. P.K., K.P., and A.N. are employees and shareholders of E.L. W.F. has received research funding to the institution from Ridgeback Biopharmaceuticals, served on adjudication committees for Janssen, Syneos, and consulted for Roche and Merck. J.J.E. is an ad hoc consultant to GSK/VIR, data monitoring committee (DMC) chair for Adagio Phase III studies. J.S.C. has consulted for Merck and Company. D.M.S. has consulted for the following companies Fluxergy, Kiadis, Linear Therapies, Matrix BioMed, Arena Pharmaceuticals, VxBiosciences, Model Medicines, Bayer Pharmaceuticals, Signant Health and Brio Clinical. All other authors (R.C., C.M., J.R., M.G., A.C.J., Y.L., M.C.C., R.D., V.B., R.M.R., A.S.P., C.V.F., and M.D.H.) report no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
