

Field validation of deep learning based Point-of-Care device for early detection of oral malignant and potentially malignant disorders
- PMID: 35995987
- PMCID: PMC9395355
- DOI: 10.1038/s41598-022-18249-x
Field validation of deep learning based Point-of-Care device for early detection of oral malignant and potentially malignant disorders
Abstract
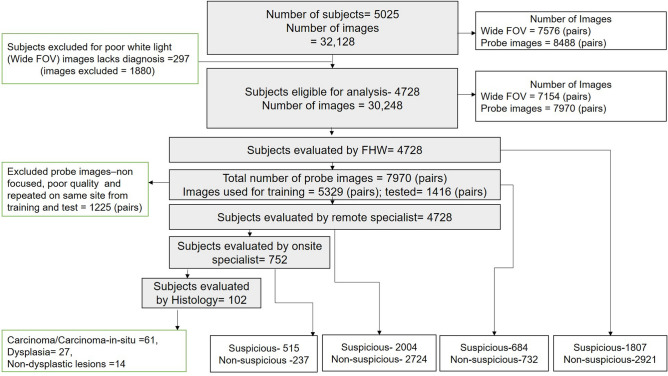
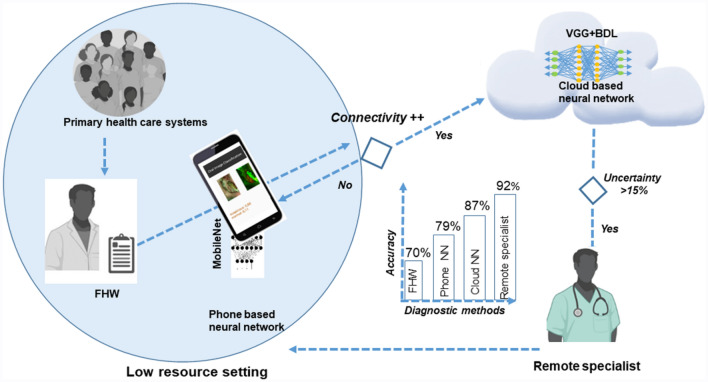
Early detection of oral cancer in low-resource settings necessitates a Point-of-Care screening tool that empowers Frontline-Health-Workers (FHW). This study was conducted to validate the accuracy of Convolutional-Neural-Network (CNN) enabled m(mobile)-Health device deployed with FHWs for delineation of suspicious oral lesions (malignant/potentially-malignant disorders). The effectiveness of the device was tested in tertiary-care hospitals and low-resource settings in India. The subjects were screened independently, either by FHWs alone or along with specialists. All the subjects were also remotely evaluated by oral cancer specialist/s. The program screened 5025 subjects (Images: 32,128) with 95% (n = 4728) having telediagnosis. Among the 16% (n = 752) assessed by onsite specialists, 20% (n = 102) underwent biopsy. Simple and complex CNN were integrated into the mobile phone and cloud respectively. The onsite specialist diagnosis showed a high sensitivity (94%), when compared to histology, while telediagnosis showed high accuracy in comparison with onsite specialists (sensitivity: 95%; specificity: 84%). FHWs, however, when compared with telediagnosis, identified suspicious lesions with less sensitivity (60%). Phone integrated, CNN (MobileNet) accurately delineated lesions (n = 1416; sensitivity: 82%) and Cloud-based CNN (VGG19) had higher accuracy (sensitivity: 87%) with tele-diagnosis as reference standard. The results of the study suggest that an automated mHealth-enabled, dual-image system is a useful triaging tool and empowers FHWs for oral cancer screening in low-resource settings.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Shah I, et al. Clinical stage of oral cancer patients at the time of initial diagnosis. J. Ayub Med. Coll. 2010;22:61–63. - PubMed
