

Comparative Validation of PlusoptiX and AI-Optic Photoscreeners in Children with High Amblyopia Risk Factor Prevalence
- PMID: 35996434
- PMCID: PMC9392476
- DOI: 10.2147/OPTH.S378777
Comparative Validation of PlusoptiX and AI-Optic Photoscreeners in Children with High Amblyopia Risk Factor Prevalence
Abstract
Purpose: In 2022, an inexpensive multi-radial infrared photoscreener, the AI Optic was released in a similar format as the 2012 PlusoptiX a-12 but utilizing artificial intelligence (AI) for online, central image interpretation. We studied them because no prior comparative validation concerning amblyopia risk factors and particularly refractive error has been done.
Patients and methods: Children from a pediatric ophthalmology practice had AI Optic and PlusoptiX-a12 photoscreen concomitantly during comprehensive examination with precisely measured strabismus and refraction. Validation to AAPOS 2021 and 2013 guidelines was evaluated with receiver operating characteristic (ROC) curves while refractive estimates were compared by the ABCD ellipsoid univariable technique.
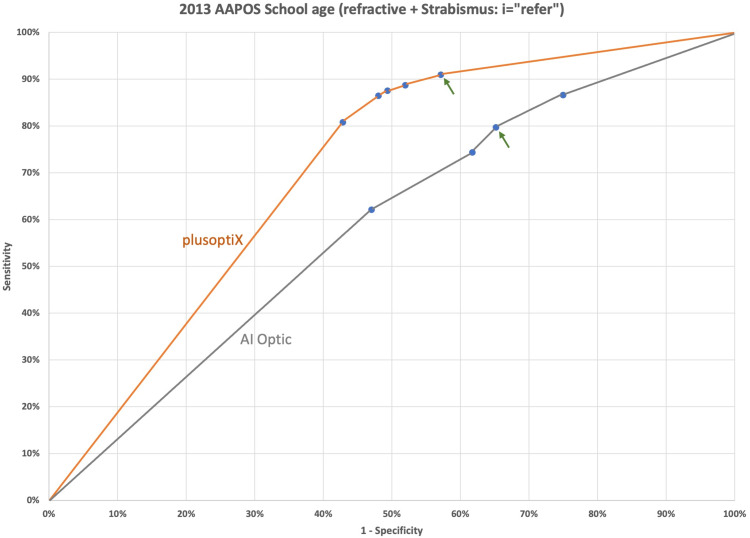
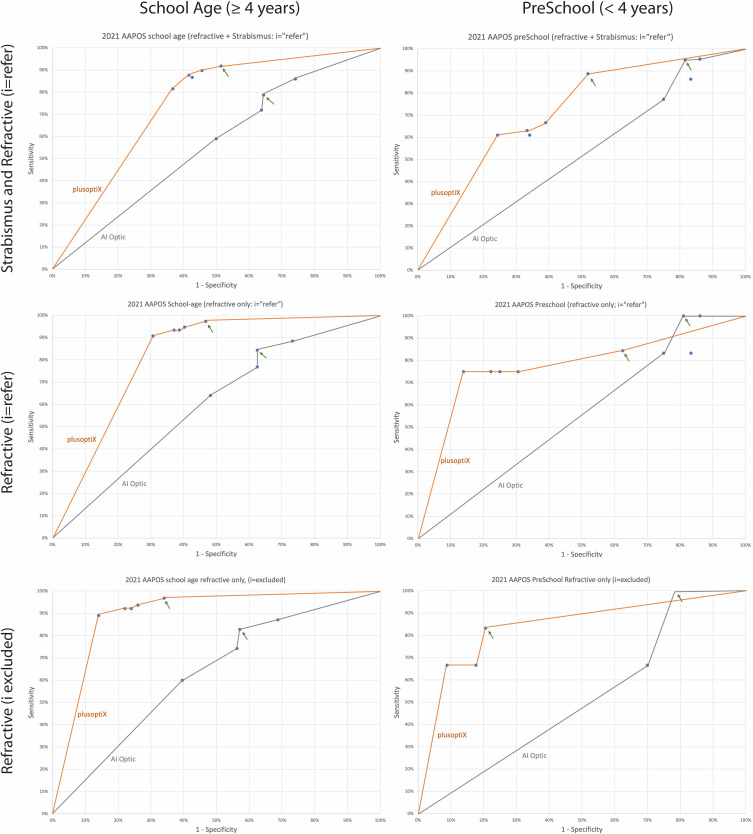
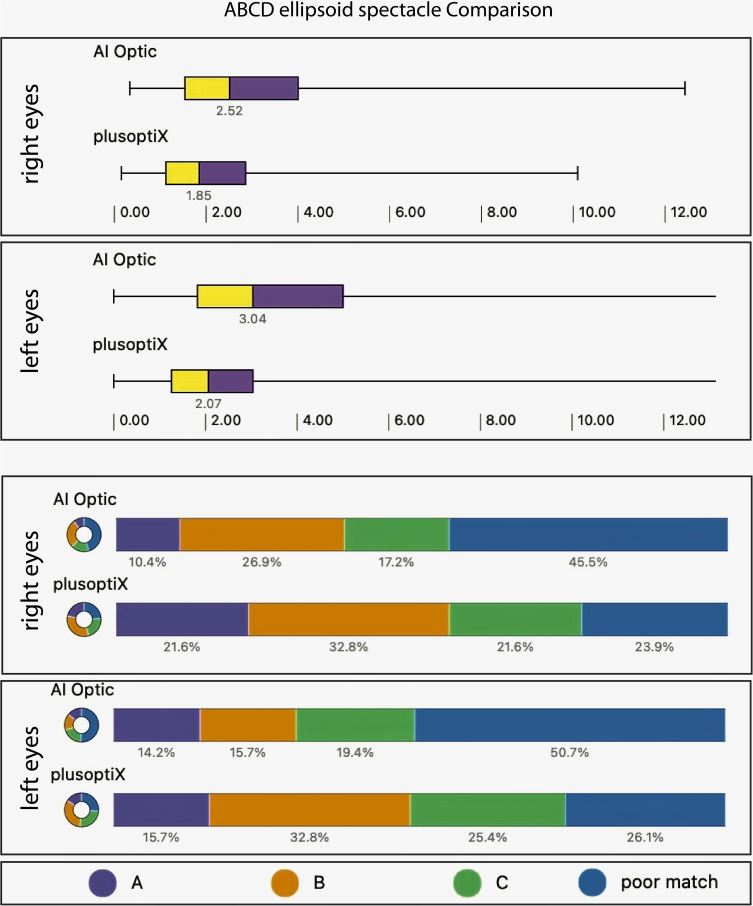
Results: In 200 ethnically diverse children aged 1-18, 148 were 4 years or older, 35% had developmental delays, and 2/3 had amblyopia risk factors (ARF). Area under the ROC curve (AUC) targeting AAPOS 2021 refractive plus strabismus for age ≥4 years was 0.58 for AI Optic and 0.74 for PlusoptiX while for children <4 years, AUC was 0.53 for AI Optic and 0.72 for PlusoptiX. For 134 comparable sphero-cylinder refractions, the ABCD Ellipsoid median (interquartile ranges) for AI Optic right eye 2.53 (1.54, 4.01) and left eye 3.05 (1.83, 5.00) did not approximate actual refraction as well as by PlusoptiX right eye 1.88 (1.12, 2.86) and left eye 2.10 (1.26, 3.04) Mann Whitney z=3.7 right and 4.2 left, p<0.001 each. AI Optic via central "AI" reading gave sphero-cylinder and referral estimates in all but 16 of 200 high risk children whereas Plusoptix had 25 inconclusives. On the other hand, with inconclusives scored as a refer, Plusoptix outperformed AI Optic in terms of ARF validation and refractive estimate.
Conclusion: Plusoptix provided more valid amblyopia and refractive screening than the cheaper AI Optic. Clinics must weigh cost versus performance, and central data sharing before selecting one of these vision-saving devices.
Keywords: amblyopia; amblyopia risk factor; photoscreening; sphero-cylinder refraction.
© 2022 Arnold.
Conflict of interest statement
Dr. Arnold coordinates the Alaska Blind Child Discovery which has received discounted vision screen technology from several vendors. He is board member of PDI Check which makes a vision screening game for autostereoscopic devices and also of Glacier Medical software which markets the cloud-based ROP screening software ROP Check. Also he is Protocol developer and Investigator for PEDIG. In addition, Dr Arnold reports unpaid advisory board member for GoCheck Kids, iScreen, Adaptica and PlusoptiX. The author reports no other conflicts of interest in this work.
Figures


Similar articles
-
Instrument Referral Criteria for PlusoptiX, SPOT and 2WIN Targeting 2021 AAPOS Guidelines.Clin Ophthalmol. 2022 Feb 25;16:489-505. doi: 10.2147/OPTH.S342666. eCollection 2022. Clin Ophthalmol. 2022. PMID: 35250260 Free PMC article.
-
Calibration and validation of the 2WIN photoscreener compared to the PlusoptiX S12 and the SPOT.J Pediatr Ophthalmol Strabismus. 2014 Sep-Oct;51(5):289-92. doi: 10.3928/01913913-20140701-01. Epub 2014 Jul 8. J Pediatr Ophthalmol Strabismus. 2014. PMID: 25000209
-
Pre-Cycloplegic Exam Benefit of Photoscreening and Accommodation-Relaxing Skiascopy.Clin Ophthalmol. 2024 Mar 15;18:833-846. doi: 10.2147/OPTH.S454430. eCollection 2024. Clin Ophthalmol. 2024. PMID: 38504935 Free PMC article.
-
Diagnostic test accuracy of Spot and Plusoptix photoscreeners in detecting amblyogenic risk factors in children: a systemic review and meta-analysis.Ophthalmic Physiol Opt. 2019 Jul;39(4):260-271. doi: 10.1111/opo.12628. Ophthalmic Physiol Opt. 2019. PMID: 31236980
-
Plusoptix photoscreener use for paediatric vision screening in Flanders and Iran.Acta Ophthalmol. 2020 Feb;98(1):80-88. doi: 10.1111/aos.14144. Epub 2019 Jun 14. Acta Ophthalmol. 2020. PMID: 31197950 Free PMC article. Review.
Cited by
-
Comparison of the PlusoptiX A16 and vision screener V100.Front Ophthalmol (Lausanne). 2024 Sep 26;4:1414417. doi: 10.3389/fopht.2024.1414417. eCollection 2024. Front Ophthalmol (Lausanne). 2024. PMID: 39391612 Free PMC article.
-
Global research of artificial intelligence in strabismus: a bibliometric analysis.Front Med (Lausanne). 2023 Sep 20;10:1244007. doi: 10.3389/fmed.2023.1244007. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37799591 Free PMC article.
References
LinkOut - more resources
Full Text Sources
