

Comparison of Diagnostic Value Between STE+LDDSE and CMR-FT for Evaluating Coronary Microvascular Obstruction in Post-PCI Patients for STEMI
- PMID: 35996553
- PMCID: PMC9391944
- DOI: 10.2147/TCRM.S374866
Comparison of Diagnostic Value Between STE+LDDSE and CMR-FT for Evaluating Coronary Microvascular Obstruction in Post-PCI Patients for STEMI
Abstract
Background: Coronary microvascular obstruction (CMVO) is closely associated with poor prognosis of ST-segment elevation myocardial infarction (STEMI) patients. However, data showing the comparison between cardiac magnetic resonance feature tracking (CMR-FT) and speckle tracking echocardiography (STE) combined with low-dose dobutamine stress echocardiography (LDDSE) in evaluating CMVO was scarcely available. We aimed to explore and compare the predictive value between CMR-FT and STE+LDDSE in detecting CMVO.
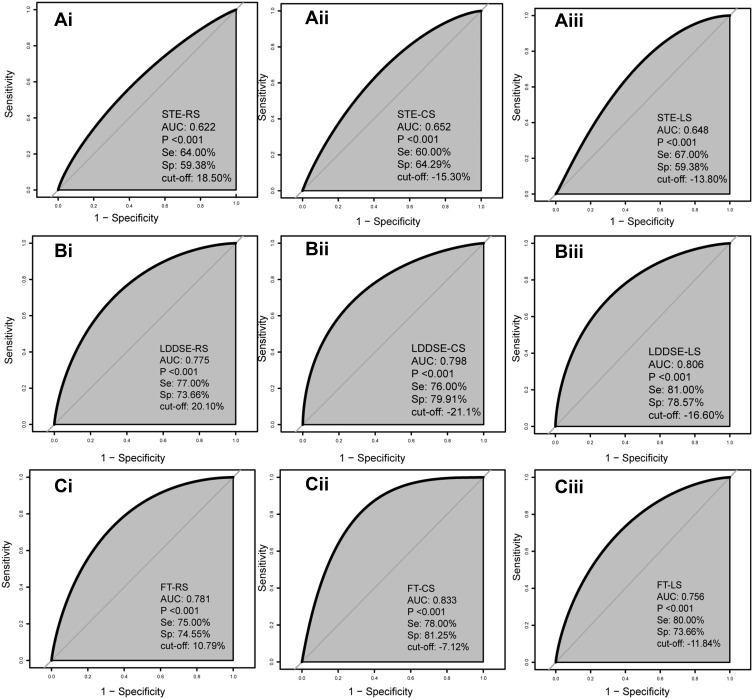
Methods: Sixty-one STEMI patients were executed cardiac magnetic resonance and echocardiography within the first 5-7 days after primary percutaneous coronary intervention (PCI). The myocardial strain analysis was performed in STE, STE+LDDSE, and CMR-FT, and strain parameters included radial strain (RS), circumferential strain (CS), and longitudinal strain (LS). ROC curves were performed to predict infarcted myocardium segments with CMVO.
Results: Finally, 324 infarcted myocardium segments were analyzed, including 100 infarcted segments with CMVO and 224 segments without CMVO by the gold standard assessment of late gadolinium-enhancement cardiac magnetic resonance imaging (LGE-CMR). The results showed that CS was generally superior to RS and LS in identifying CMVO. CS in CMR-FT facilitated the detection of CMVO, with a sensitivity, specificity, and accuracy of 78.00%, 81.25%, and 80.25%, respectively. The sensitivity, specificity, and accuracy of CS in STE combined with LDDSE were better than STE alone (76.00% vs 60.00%, 79.91% vs 64.29%, and 78.70% vs 62.96%, P < 0.05). In addition, CMR-FT is not superior to STE+LDDSE for detection of CMVO (P > 0.05).
Conclusion: Low-dose dobutamine can improve the clinical value of STE for evaluating CMVO in STEMI patients. Compared with CMR-FT, STE+LDDSE might be a better choice for STEMI patients because of its safety, convenience, and low-cost.
Keywords: ST-segment elevation myocardial infarction; coronary microvascular obstruction; low-dose dobutamine; magnetic resonance feature tracking; speckle tracking echocardiography.
© 2022 Liu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures


Similar articles
-
Direct comparison of coronary microvascular obstruction evaluation using CMR feature tracking and layer-specific speckle tracking echocardiography in STEMI patients.Int J Cardiovasc Imaging. 2024 Feb;40(2):237-247. doi: 10.1007/s10554-023-02998-5. Epub 2023 Nov 13. Int J Cardiovasc Imaging. 2024. PMID: 37953371 Free PMC article.
-
Predictive Value of Cardiac Magnetic Resonance Feature Tracking after Acute Myocardial Infarction: A Comparison with Dobutamine Stress Echocardiography.J Clin Med. 2021 Nov 12;10(22):5261. doi: 10.3390/jcm10225261. J Clin Med. 2021. PMID: 34830543 Free PMC article.
-
The evaluation of coronary microvascular obstruction in patients with STEMI by cardiac magnetic resonance T2-STIR image and layer-specific analysis of 2-dimensional speckle tracking echocardiography combined with low-dose dobutamine stress echocardiography.Heart Vessels. 2023 Jan;38(1):40-48. doi: 10.1007/s00380-022-02131-x. Epub 2022 Aug 1. Heart Vessels. 2023. PMID: 35915265
-
Coronary microvascular obstruction and dysfunction in patients with acute myocardial infarction.Nat Rev Cardiol. 2024 May;21(5):283-298. doi: 10.1038/s41569-023-00953-4. Epub 2023 Nov 24. Nat Rev Cardiol. 2024. PMID: 38001231 Review.
-
Mechanism of Coronary Microcirculation Obstruction after Acute Myocardial Infarction and Cardioprotective Strategies.Rev Cardiovasc Med. 2024 Oct 12;25(10):367. doi: 10.31083/j.rcm2510367. eCollection 2024 Oct. Rev Cardiovasc Med. 2024. PMID: 39484142 Free PMC article. Review.
Cited by
-
Direct comparison of coronary microvascular obstruction evaluation using CMR feature tracking and layer-specific speckle tracking echocardiography in STEMI patients.Int J Cardiovasc Imaging. 2024 Feb;40(2):237-247. doi: 10.1007/s10554-023-02998-5. Epub 2023 Nov 13. Int J Cardiovasc Imaging. 2024. PMID: 37953371 Free PMC article.
-
Applications of Speckle Tracking Echocardiography in Stress Echocardiography: A Systematic Review on Feasibility, Diagnostic, and Clinical Utility.Echocardiography. 2025 Aug;42(8):e70251. doi: 10.1111/echo.70251. Echocardiography. 2025. PMID: 40767309 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
