

Vaginal repair of cesarean section scar defects: Preoperative hysteroscopic evaluation
- PMID: 35996831
- PMCID: PMC9851086
- DOI: 10.1111/aogs.14429
Vaginal repair of cesarean section scar defects: Preoperative hysteroscopic evaluation
Abstract
Introduction: Cesarean section scar defects (CSDs) are one of the long-term complications following cesarean section. They can be detected by transvaginal sonography, hysterosalpingography, sonohysterography and magnetic resonance imaging (MRI). Hysteroscopy is frequently used in evaluating endometrial disease. However, the description of CSDs by hysteroscopy is very limited. Only a few papers about hysteroscopy evaluation have been published. This is an exploratory study to compare hysteroscopic findings with myometrial thickness and post-surgical outcomes.
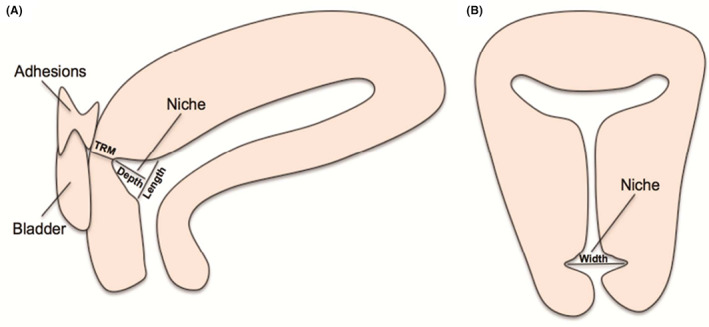
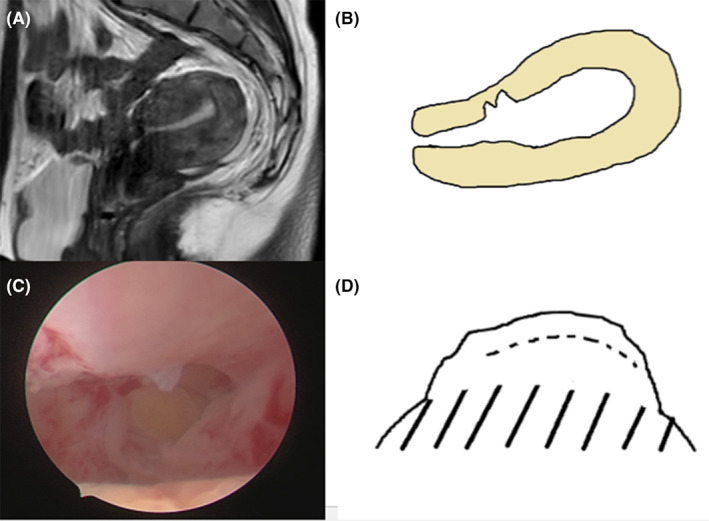
Material and methods: From February 2019 to December 2020, 143 women with CSDs were enrolled in the observational study. All women suffered from abnormal uterine bleeding and were evaluated in a standardized way with hysteroscopy before vaginal surgery. Dome-shaped CSDs could be clearly observed in all patients under hysteroscopy. We recorded the pictures of each patient under hysteroscopy and classified them. All patients underwent outpatient review at 3 and 6 months after surgery to obtain menstrual information and CSD scar size by MRI or transvaginal sonography.
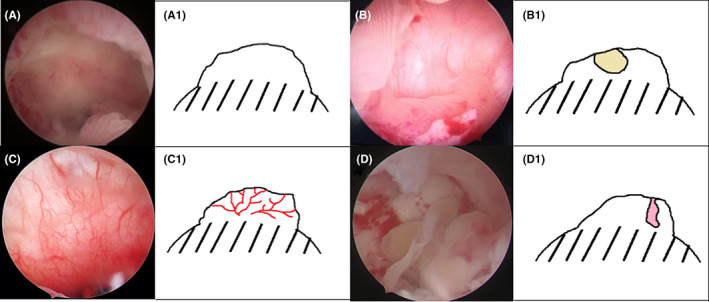
Results: Pale mucosae in the defect were meager endometrial lining covering the surface of muscle layer, cyst lesions were some cyst lesions in the defect, increased local vascularization was a vascular tree with branching and irregular vascular distribution in defect, polypoid lesions were polypoid lesions in the defect, and serrated niches were two niches at the anterior uterine isthmus. The features of the CSDs observed under hysteroscopy were identified as five phenotypes: pale mucosae (90/143, 62.9%), cyst lesions (23/143, 16.1%), polypoid lesions (19/143, 13.3%), increased local vascularization (27/143, 18.9%) and serrated niches (7/143, 4.9%). The most common finding in scar defects under hysteroscopy was pale mucosae in the CSD. The results suggest that patients with increased local vascularization and serrated niches have a high risk of thinner residual myometrium before vaginal repair (p < 0.05). However, there was no significant difference in menstrual duration or in the outcome of vaginal repair for CSDs between these five phenotypes (p > 0.05).
Conclusions: Patients with the abnormal blood vessel or serration phenotypes of defects under hysteroscopy may have a thinner residual myometrium. The phenotypes of hysteroscopic findings of CSDs have no correlation with the outcome of repair.
Keywords: cesarean section scar defect; hysteroscopy; myometrial thickness; surgical outcomes.
© 2022 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Figures
Similar articles
-
Hysteroscopic removal, with or without laparoscopic assistance, of first-trimester cesarean scar pregnancy.Fertil Steril. 2022 Mar;117(3):643-645. doi: 10.1016/j.fertnstert.2021.11.027. Fertil Steril. 2022. PMID: 35219475
-
Clinical Success Rate of Extensive Hysteroscopic Cesarean Scar Defect Excision and Correlation to Histologic Findings.J Minim Invasive Gynecol. 2020 Jan;27(1):129-134. doi: 10.1016/j.jmig.2019.03.001. Epub 2019 Mar 8. J Minim Invasive Gynecol. 2020. PMID: 30858053
-
Hysteroscopy-assisted Transvaginal Repair without Scar Defect Resection: A Novel Technique for the Treatment of Uterine Niche.J Minim Invasive Gynecol. 2023 Mar;30(3):178-179. doi: 10.1016/j.jmig.2023.01.004. Epub 2023 Jan 14. J Minim Invasive Gynecol. 2023. PMID: 36646313
-
Cesarean scar defects: management of an iatrogenic pathology whose prevalence has dramatically increased.Fertil Steril. 2020 Apr;113(4):704-716. doi: 10.1016/j.fertnstert.2020.01.037. Fertil Steril. 2020. PMID: 32228874 Review.
-
Cesarean scar disorder: Management and repair.Best Pract Res Clin Obstet Gynaecol. 2023 Aug;90:102398. doi: 10.1016/j.bpobgyn.2023.102398. Epub 2023 Aug 4. Best Pract Res Clin Obstet Gynaecol. 2023. PMID: 37598564 Review.
Cited by
-
Value and influencing factors of preoperative MRI evaluation for previous cesarean scar defect associated abnormal uterine bleeding in patients undergoing laparoscopic surgery.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023 Sept 28;48(9):1316-1324. doi: 10.11817/j.issn.1672-7347.2023.230123. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2023. PMID: 38044642 Free PMC article.
-
Accuracy of multimodal vaginal ultrasound in the detection and assessment of scar healing after caesarean section: a correlational meta-analysis.Ann Med. 2025 Dec;57(1):2523558. doi: 10.1080/07853890.2025.2523558. Epub 2025 Jun 30. Ann Med. 2025. PMID: 40587769 Free PMC article. Review.
-
Treatment of Cesarean Scar Ectopic Pregnancy with Hysteroscopic Resection.Gynecol Minim Invasive Ther. 2025 Mar 15;14(2):170-173. doi: 10.4103/gmit.gmit_28_24. eCollection 2025 Apr-Jun. Gynecol Minim Invasive Ther. 2025. PMID: 40521575 Free PMC article.
-
Clinical analysis of uterine parameters evaluated by preoperative magnetic resonance imaging in patients treated by hysteroscopic approach with previous cesarean scar defect-related abnormal uterine bleeding: a retrospective cohort study.Quant Imaging Med Surg. 2024 Mar 15;14(3):2334-2344. doi: 10.21037/qims-23-1205. Epub 2024 Mar 1. Quant Imaging Med Surg. 2024. PMID: 38545049 Free PMC article.
-
Prevalence, definition, and etiology of cesarean scar defect and treatment of cesarean scar disorder: A narrative review.Reprod Med Biol. 2023 Aug 9;22(1):e12532. doi: 10.1002/rmb2.12532. eCollection 2023 Jan-Dec. Reprod Med Biol. 2023. PMID: 37577060 Free PMC article. Review.
References
-
- Walker R, Turnbull D, Wilkinson C. Strategies to address global cesarean section rates: a review of the evidence. Birth. 2002;29:28‐39. - PubMed
-
- Molina G, Weiser TG, Lipsitz SR, et al. Relationship between cesarean delivery rate and maternal and neonatal mortality. JAMA. 2015;314:2263‐2270. - PubMed
-
- Fabres C, Aviles G, De La Jara C, et al. The cesarean delivery scar pouch: clinical implications and diagnostic correlation between transvaginal sonography and hysteroscopy. J Ultrasound Med. 2003;22:695‐700; quiz 701‐2. - PubMed
-
- Vikhareva Osser O, Valentin L. Clinical importance of appearance of cesarean hysterotomy scar at transvaginal ultrasonography in nonpregnant women. Obstet Gynecol. 2011;117:525‐532. - PubMed
-
- Tower AM, Frishman GN. Cesarean scar defects: an underrecognized cause of abnormal uterine bleeding and other gynecologic complications. J Minim Invasive Gynecol. 2013;20:562‐572. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
