

Differential airway remodeling changes were observed in patients with asthma COPD overlap compared to patients with asthma and COPD alone
- PMID: 35997281
- PMCID: PMC9550567
- DOI: 10.1152/ajplung.00137.2022
Differential airway remodeling changes were observed in patients with asthma COPD overlap compared to patients with asthma and COPD alone
Abstract
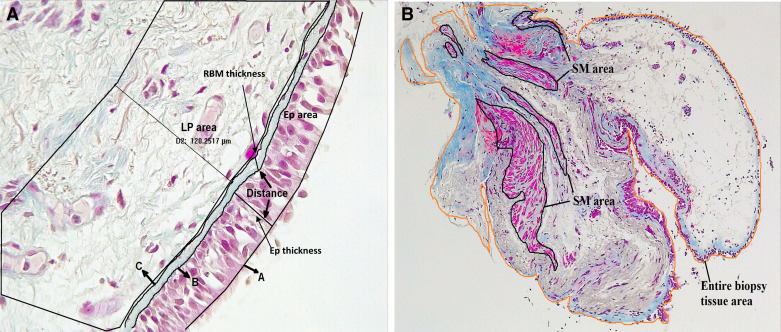
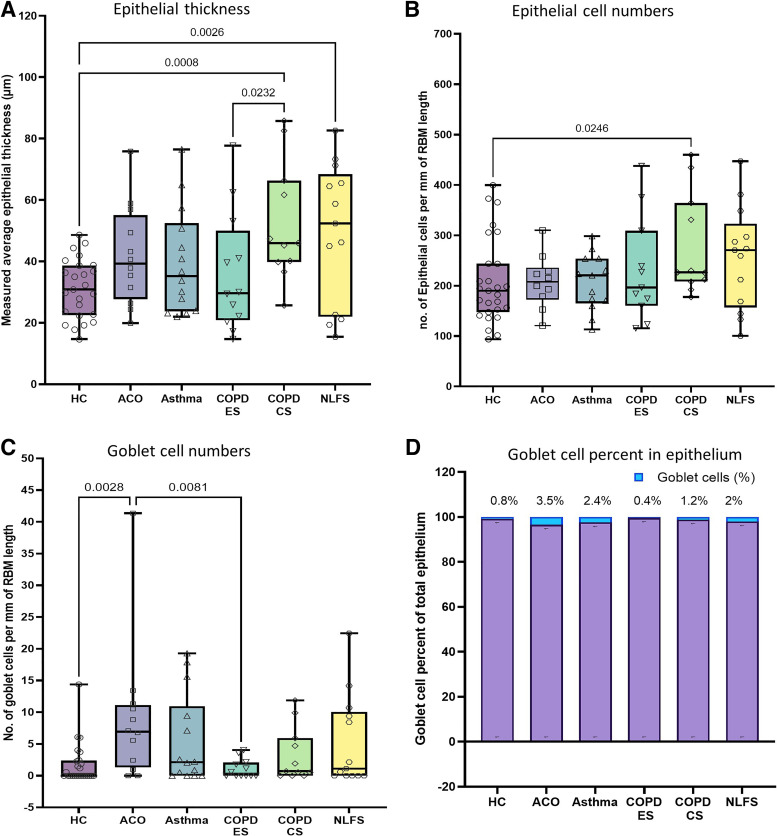
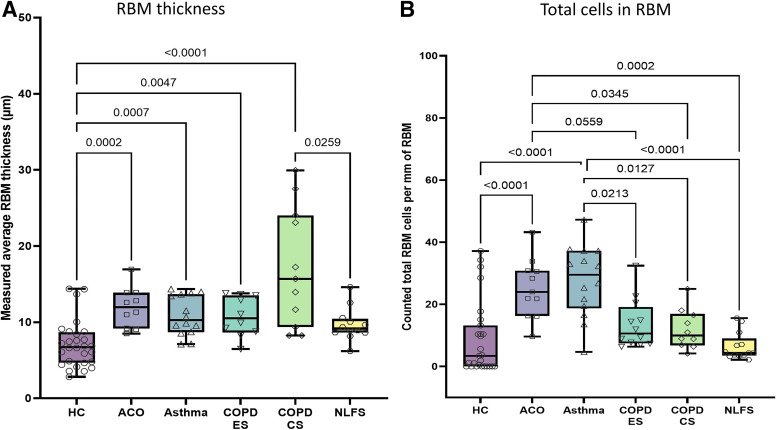
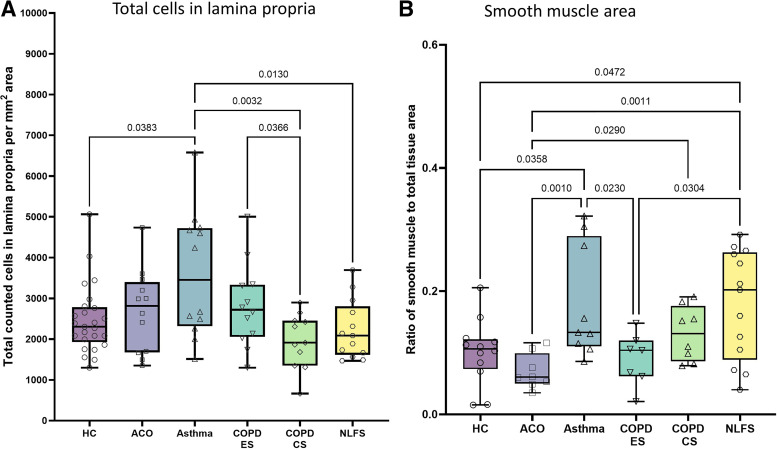
Management of patients with asthma COPD overlap (ACO) is clinically challenging due to insufficient evidence of pathological changes in these patients. In this cross-sectional study, we evaluated airway remodeling in endobronchial biopsies from a total of 90 subjects, which included 12 ACO, 14 patients with asthma, 12 COPD exsmokers (ES), 11 current smokers (CS), 28 healthy controls (HC), and 13 normal lung function smokers (NLFS). Tissue was stained with Masson's trichrome. Epithelium, goblet cells, reticular basement membrane (RBM), cellularity, lamina propria (LP), and smooth muscle (SM) changes were measured using Image-Pro Plus v7 software. Differential airway remodeling pattern was seen in patients with ACO. A limited change was noted in the ACO epithelium compared with other pathological groups. RBM was substantially thicker in patients with ACO than in HC (P < 0.0002) and tended to be thicker than in patients with asthma and NLFS. The total RBM cells were higher in ACO than in the HC (P < 0.0001), COPD-CS (P = 0.0559), -ES (P = 0.0345), and NLFS (P < 0.0002), but did not differ from patients with asthma. Goblet cells were higher in the ACO than in the HC (P = 0.0028) and COPD-ES (P = 0.0081). The total LP cells in ACO appeared to be higher than in HC, COPD-CS, and NLFS but appeared to be lower than in patients with asthma. Finally, SM area was significantly lower in the ACO than in patients with asthma (P = 0.001), COPD-CS (=0.0290), and NLFS (P = 0.0011). This first comprehensive study suggests that patients with ACO had distinguishable tissue remodeling that appeared to be more severe than patients with asthma and COPD. This study will help in informed decision-making for better patient management in clinical practice.
Keywords: COPD; airway remodeling; asthma; asthma COPD overlap; smoking.
Conflict of interest statement
S. S. Sohal reports personal fees from Chiesi outside the submitted work. None of the other authors has any conflicts of interest, financial or otherwise, to disclose.
Figures

References
-
- Global Initiative for Asthma. Global Strategy for asthma management and prevention [Online]. www.ginasthma.org [2021 Jan 05].
-
- Global Initiative For Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease [Online]. https://goldcopd.org/ [2021 Jan 05].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical