

Effect of Radiotherapy Alone vs Radiotherapy With Concurrent Chemoradiotherapy on Survival Without Disease Relapse in Patients With Low-risk Nasopharyngeal Carcinoma: A Randomized Clinical Trial
- PMID: 35997729
- PMCID: PMC9399866
- DOI: 10.1001/jama.2022.13997
Effect of Radiotherapy Alone vs Radiotherapy With Concurrent Chemoradiotherapy on Survival Without Disease Relapse in Patients With Low-risk Nasopharyngeal Carcinoma: A Randomized Clinical Trial
Abstract
Importance: Concurrent chemoradiotherapy has been the standard treatment for stage II nasopharyngeal carcinoma (NPC) based on data using 2-dimensional conventional radiotherapy. There is limited evidence for the role of chemotherapy with use of intensity-modulated radiation therapy (IMRT).
Objective: To assess whether concurrent chemotherapy can be safely omitted for patients with low-risk stage II/T3N0 NPC treated with IMRT.
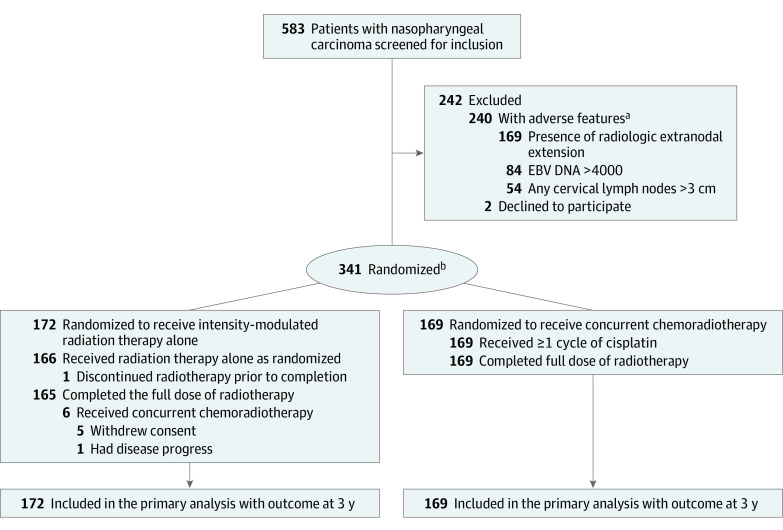
Design, setting, and participants: This multicenter, open-label, randomized, phase 3, noninferiority clinical trial was conducted at 5 Chinese hospitals, including 341 adult patients with low-risk NPC, defined as stage II/T3N0M0 without adverse features (all nodes <3 cm, no level IV/Vb nodes; no extranodal extension; Epstein-Barr virus DNA <4000 copies/mL), with enrollment between November 2015 and August 2020. The final date of follow-up was March 15, 2022.
Interventions: Patients were randomly assigned to receive IMRT alone (n = 172) or concurrent chemoradiotherapy (IMRT with cisplatin, 100 mg/m2 every 3 weeks for 3 cycles [n = 169]).
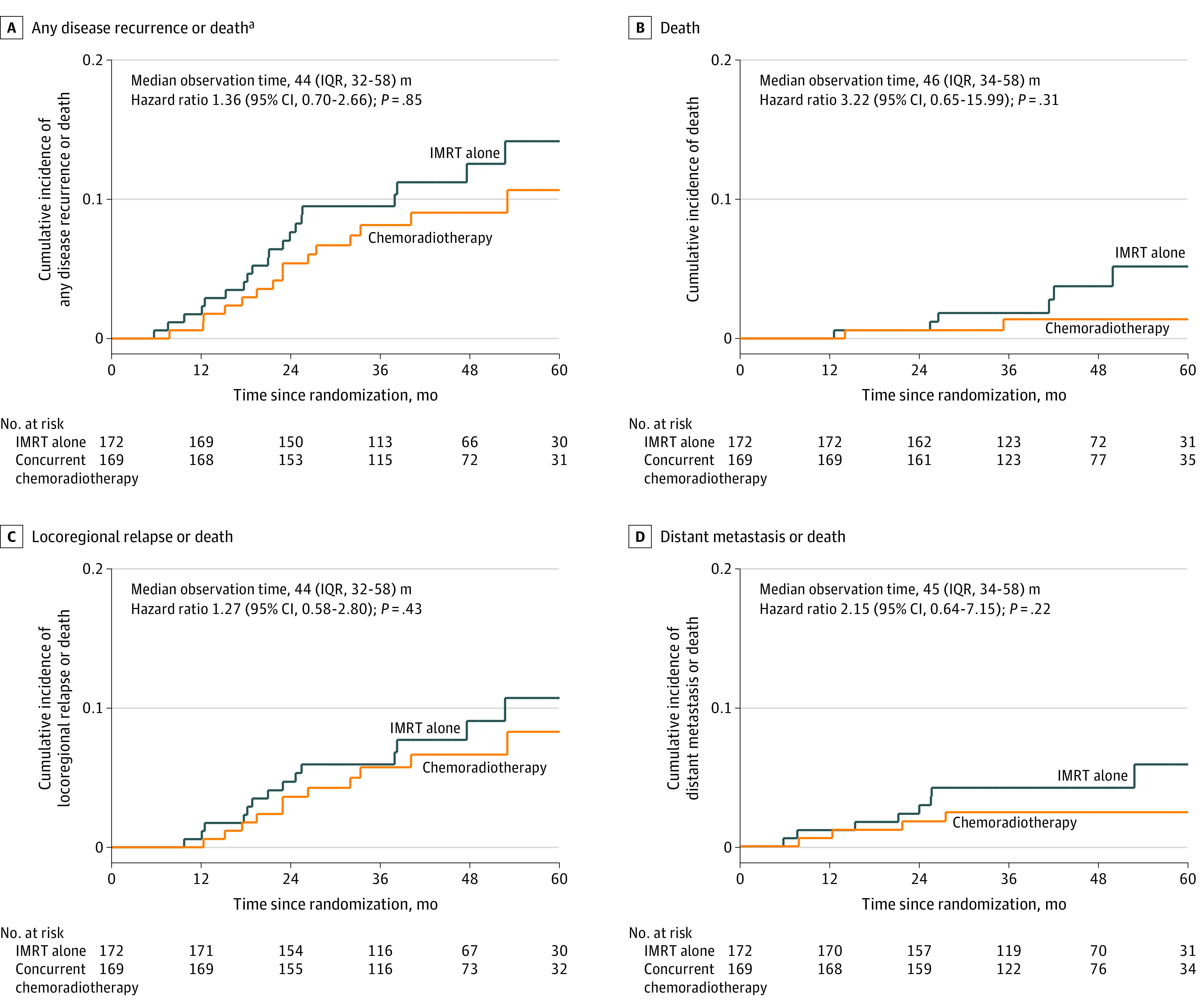
Main outcomes and measures: The primary end point was 3-year failure-free survival (time from randomization to any disease relapse or death), with a noninferiority margin of 10%. Secondary end points comprised overall survival, locoregional relapse-free survival, distant metastasis-free survival, adverse events, and health-related quality of life (QOL) measured by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (QLQ-C30; range, 0-100 points; minimum clinically important difference ≥10 for physical function, symptom control, or health-related QOL; higher score indicates better functioning and global health status or worse symptoms).
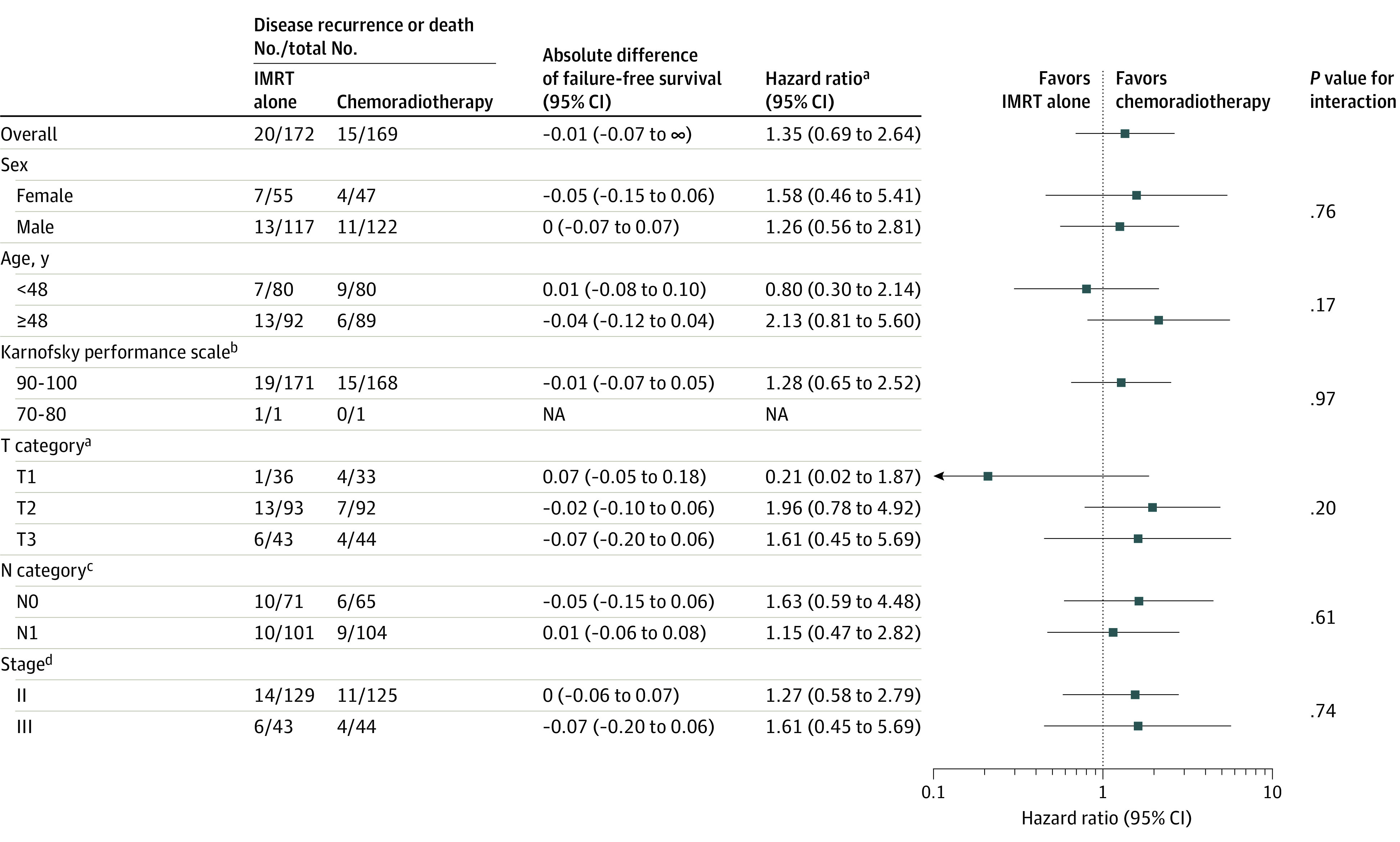
Results: Among 341 randomized patients (mean [SD] age, 48 [10] years; 30% women), 334 (98.0%) completed the trial. Median follow-up was 46 months (IQR, 34-58). Three-year failure-free survival was 90.5% for the IMRT-alone group vs 91.9% for the concurrent chemoradiotherapy group (difference, -1.4%; 1-sided 95% CI, -7.4% to ∞; P value for noninferiority, <.001). No significant differences were observed between groups in overall survival, locoregional relapse, or distant metastasis. The IMRT-alone group experienced a significantly lower incidence of grade 3 to 4 adverse events (17% vs 46%; difference, -29% [95% CI, -39% to -20%]), including hematologic toxicities (leukopenia, neutropenia) and nonhematologic toxicities (nausea, vomiting, anorexia, weight loss, mucositis). The IMRT-alone group had significantly better QOL scores during radiotherapy including the domains of global health status, social functioning, fatigue, nausea and vomiting, pain, insomnia, appetite loss, and constipation.
Conclusions and relevance: Among patients with low-risk NPC, treatment with IMRT alone resulted in 3-year failure-free survival that was not inferior to concurrent chemoradiotherapy.
Trial registration: ClinicalTrials.gov Identifier: NCT02633202.
Conflict of interest statement
Figures
Comment in
-
Radiotherapy Alone vs Radiotherapy With Concurrent Chemoradiotherapy and Survival of Patients With Low-Risk Nasopharyngeal Carcinoma.JAMA. 2023 Jan 17;329(3):261. doi: 10.1001/jama.2022.21033. JAMA. 2023. PMID: 36648473 No abstract available.
-
Radiotherapy Alone vs Radiotherapy With Concurrent Chemoradiotherapy and Survival of Patients With Low-Risk Nasopharyngeal Carcinoma.JAMA. 2023 Jan 17;329(3):260. doi: 10.1001/jama.2022.21030. JAMA. 2023. PMID: 36648474 No abstract available.
-
Radiotherapy Alone vs Radiotherapy With Concurrent Chemoradiotherapy and Survival of Patients With Low-Risk Nasopharyngeal Carcinoma.JAMA. 2023 Jan 17;329(3):260-261. doi: 10.1001/jama.2022.21027. JAMA. 2023. PMID: 36648475 No abstract available.
References
-
- Lee AW, Lau WH, Tung SY, et al. ; Hong Kong Nasopharyngeal Cancer Study Group . Preliminary results of a randomized study on therapeutic gain by concurrent chemotherapy for regionally-advanced nasopharyngeal carcinoma: NPC-9901 trial by the Hong Kong Nasopharyngeal Cancer Study Group. J Clin Oncol. 2005;23(28):6966-6975. doi:10.1200/JCO.2004.00.7542 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
