

Temporal development of T cell receptor repertoires during childhood in health and disease
- PMID: 35998036
- PMCID: PMC9675557
- DOI: 10.1172/jci.insight.161885
Temporal development of T cell receptor repertoires during childhood in health and disease
Abstract
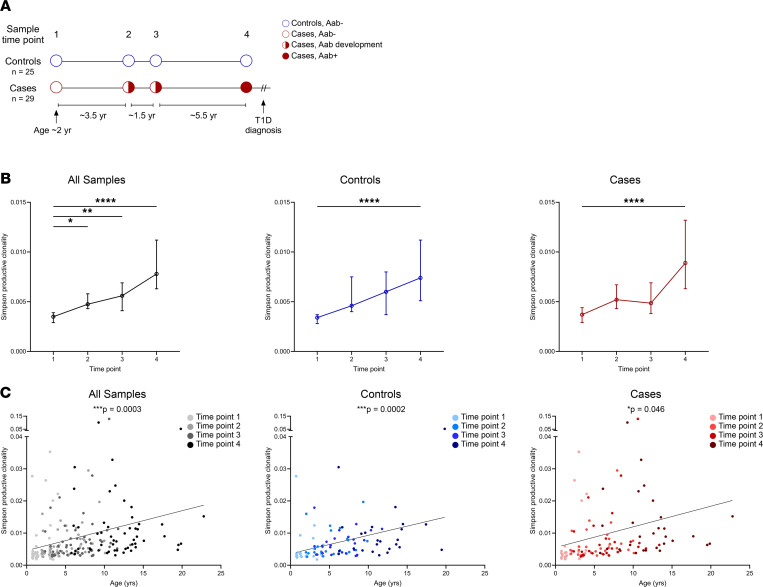
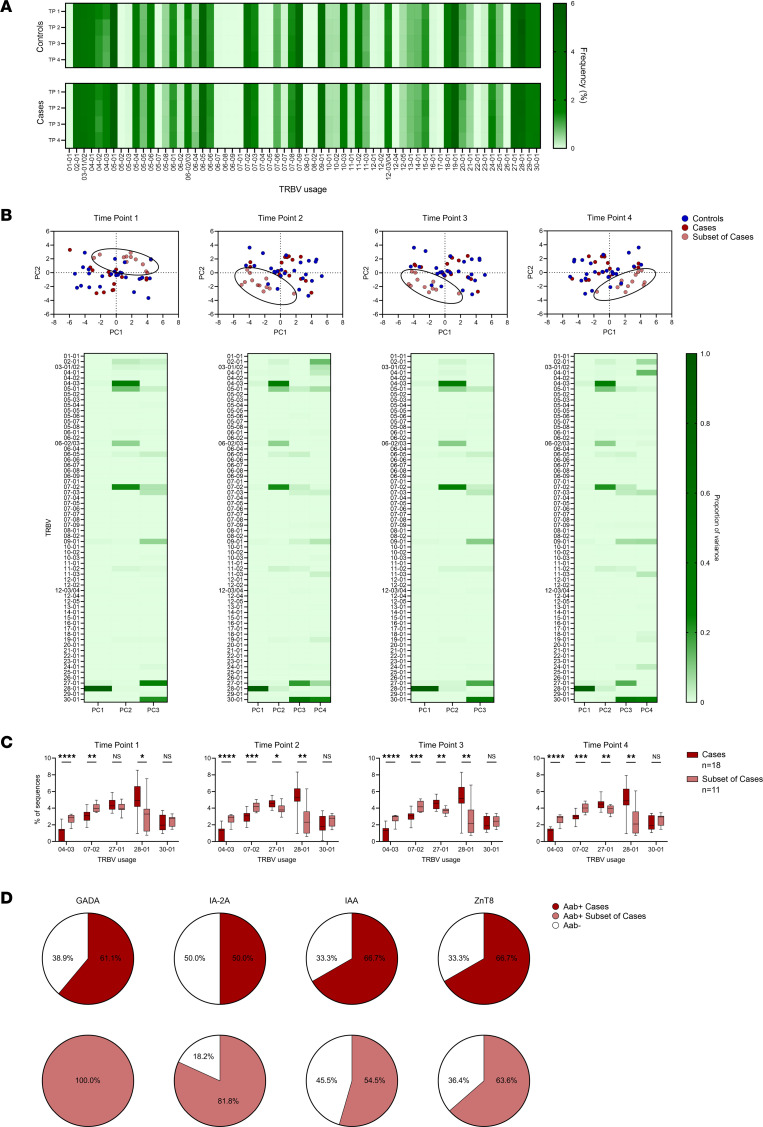
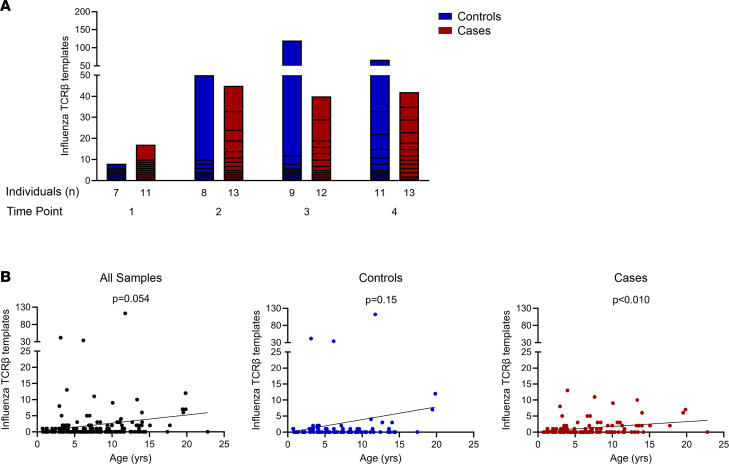
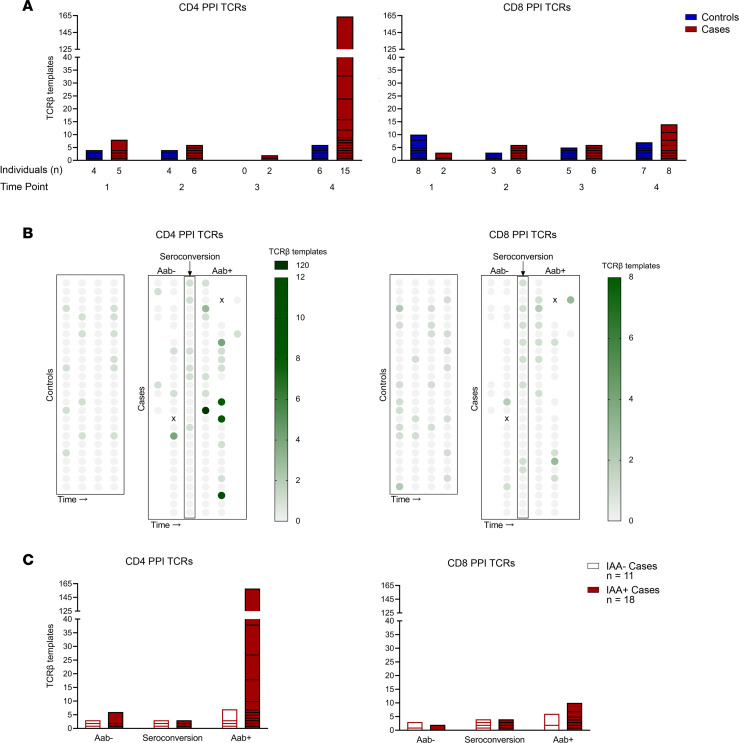
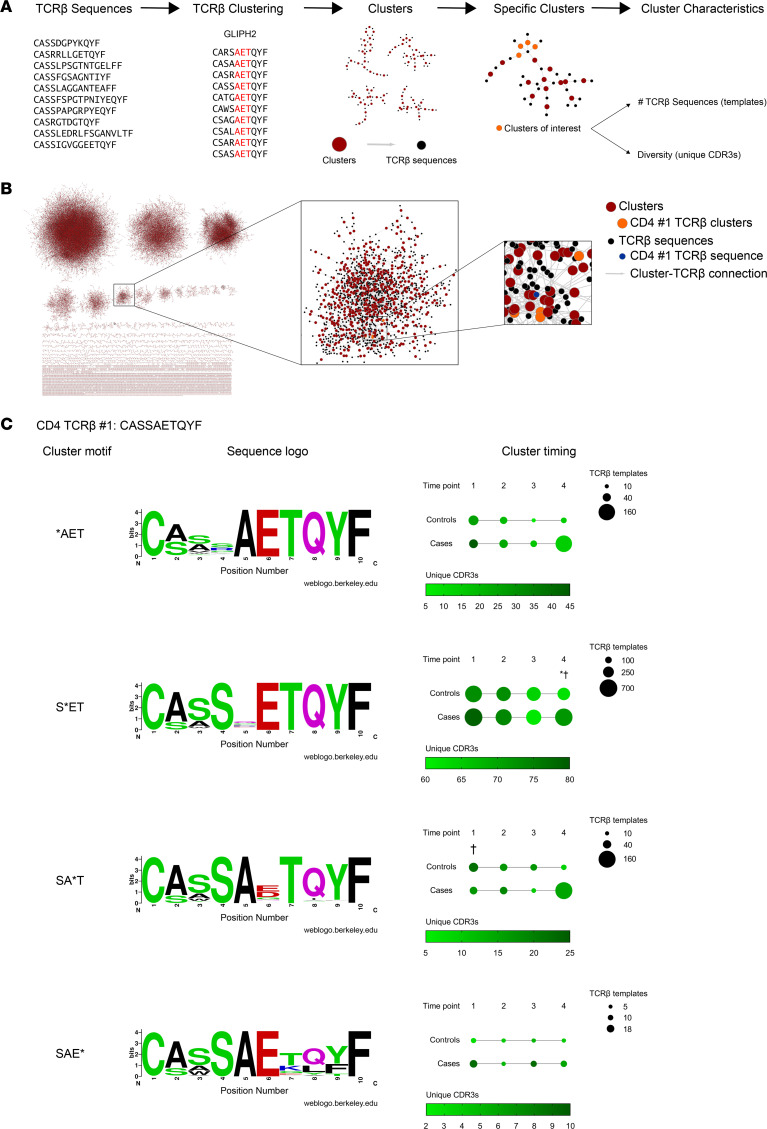
T cell receptor (TCR) sequences are exceptionally diverse and can now be comprehensively measured with next-generation sequencing technologies. However, a thorough investigation of longitudinal TCR repertoires throughout childhood in health and during development of a common childhood disease, type 1 diabetes (T1D), has not been undertaken. Here, we deep sequenced the TCR-β chain repertoires from longitudinal peripheral blood DNA samples at 4 time points beginning early in life (median age of 1.4 years) from children who progressed to T1D (n = 29) and age/sex-matched islet autoantibody-negative controls (n = 25). From 53 million TCR-β sequences, we show that the repertoire is extraordinarily diverse early in life and narrows with age independently of disease. We demonstrate the ability to identify specific TCR sequences, including those known to recognize influenza A and, separately, those specific for insulin and its precursor, preproinsulin. Insulin-reactive TCR-β sequences were more common and frequent in number as the disease progressed in those who developed T1D compared with genetically at risk nondiabetic children, and this was not the case for influenza-reactive sequences. As an independent validation, we sequenced and analyzed TCR-β repertoires from a cohort of new-onset T1D patients (n = 143), identifying the same preproinsulin-reactive TCRs. These results demonstrate an enrichment of preproinsulin-reactive TCR sequences during the progression to T1D, highlighting the importance of using disease-relevant TCR sequences as powerful biomarkers in autoimmune disorders.
Keywords: Adaptive immunity; Autoimmunity; Diabetes; Immunology; T cell receptor.
Conflict of interest statement
Figures
References
-
- Huppa JB, Davis MM. The interdisciplinary science of T-cell recognition. Adv Immunol. 2013;119:1–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
