

Hyperphosphatemia and its relationship with blood pressure, vasoconstriction, and endothelial cell dysfunction in hypertensive hemodialysis patients
- PMID: 35999520
- PMCID: PMC9396889
- DOI: 10.1186/s12882-022-02918-0
Hyperphosphatemia and its relationship with blood pressure, vasoconstriction, and endothelial cell dysfunction in hypertensive hemodialysis patients
Abstract
Background: Hyperphosphatemia occurs frequently in end-stage renal disease patients on hemodialysis and is associated with increased mortality. Hyperphosphatemia contributes to vascular calcification in these patients, but there is emerging evidence that it is also associated with endothelial cell dysfunction.
Methods: We conducted a cross-sectional study in hypertensive hemodialysis patients. We obtained pre-hemodialysis measurements of total peripheral resistance index (TPRI, non-invasive cardiac output monitor) and plasma levels of endothelin-1 (ET-1) and asymmetric dimethylarginine (ADMA). We ascertained the routine peridialytic blood pressure (BP) measurements from that treatment and the most recent pre-hemodialysis serum phosphate levels. We used generalized linear regression analyses to determine independent associations between serum phosphate with BP, TPRI, ET-1, and ADMA while controlling for demographic variables, parathyroid hormone (PTH), and interdialytic weight gain.
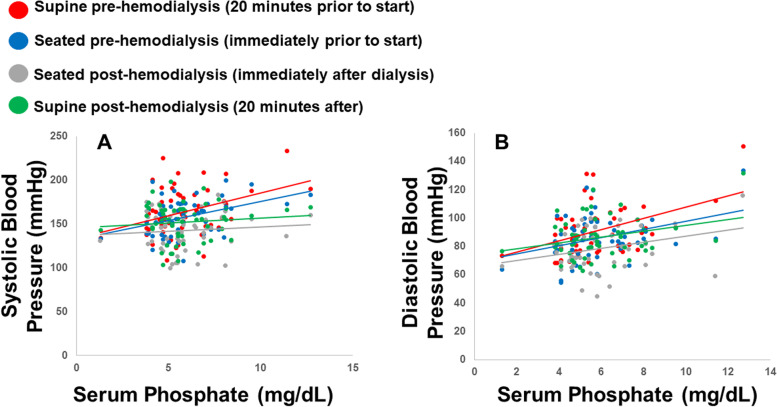
Results: There were 54 patients analyzed. Mean pre-HD supine and seated systolic and diastolic BP were 164 (27), 158 (21), 91.5 (17), and 86.1 (16) mmHg. Mean serum phosphate was 5.89 (1.8) mg/dL. There were significant correlations between phosphate with all pre-hemodialysis BP measurements (r = 0.3, p = .04; r = 0.4, p = .002; r = 0.5, p < .0001; and r = 0.5, p = .0003.) The correlations with phosphate and TPRI, ET-1, and ADMA were 0.3 (p = .01), 0.4 (p = .007), and 0.3 (p = .04). In our final linear regression analyses controlling for baseline characteristics, PTH, and interdialytic weight gain, independent associations between phosphate with pre-hemodialysis diastolic BP, TPRI, and ET-1 were retained (β = 4.33, p = .0002; log transformed β = 0.05, p = .005; reciprocal transformed β = -0.03, p = .047).
Conclusions: Serum phosphate concentration is independently associated with higher pre-HD BP, vasoconstriction, and markers of endothelial cell dysfunction. These findings demonstrate an additional negative impact of hyperphosphatemia on cardiovascular health beyond vascular calcification.
Trial registration: The study was part of a registered clinical trial, NCT01862497 (May 24, 2013).
Keywords: Endothelial cell dysfunction; Hemodialysis; Mineral bone disease; Phosphate; Vasoconstriction.
© 2022. The Author(s).
Conflict of interest statement
Dr. Van Buren serves on the Editorial Board for BMC Nephrology, but there are no significant financial or non-financial competing interests.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
