

Palliative psychiatry in a narrow and in a broad sense: A concept clarification
- PMID: 35999690
- PMCID: PMC9679794
- DOI: 10.1177/00048674221114784
Palliative psychiatry in a narrow and in a broad sense: A concept clarification
Abstract
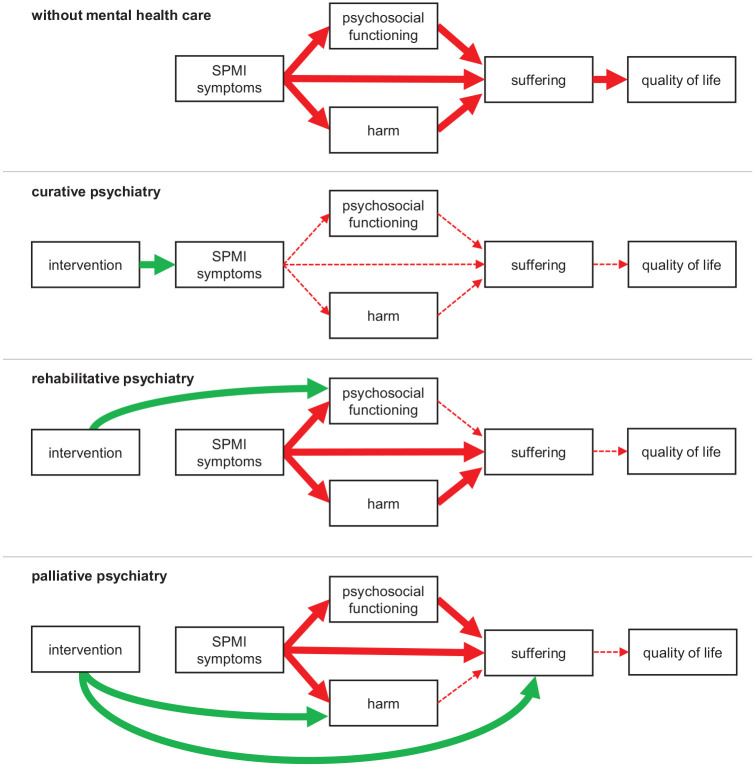
Even with optimal treatment, some persons with severe and persistent mental illness do not achieve a level of mental health, psychosocial functioning and quality of life that is acceptable to them. With each unsuccessful treatment attempt, the probability of achieving symptom reduction declines while the probability of somatic and psychological side effects increases. This worsening benefit-harm ratio of treatment aiming at symptom reduction has motivated calls for implementing palliative approaches to care into psychiatry (palliative psychiatry). Palliative psychiatry accepts that some cases of severe and persistent mental illness can be irremediable and calls for a careful evaluation of goals of care in these cases. It aims at reducing harm, relieving suffering and thus improving quality of life directly, working around irremediable psychiatric symptoms. In a narrow sense, this refers to patients likely to die of their severe and persistent mental illness soon, but palliative psychiatry in a broad sense is not limited to end-of-life care. It can - and often should - be integrated with curative and rehabilitative approaches, as is the gold standard in somatic medicine. Palliative psychiatry constitutes a valuable addition to established non-curative approaches such as rehabilitative psychiatry (which focuses on psychosocial functioning instead of quality of life) and personal recovery (a journey that persons living with severe and persistent mental illness may undertake, not necessarily accompanied by mental health care professionals). Although the implementation of palliative psychiatry is met with several challenges such as difficulties regarding decision-making capacity and prognostication in severe and persistent mental illness, it is a promising new approach in caring for persons with severe and persistent mental illness, regardless of whether they are at the end of life.
Keywords: Severe and persistent mental illness; end of life; futility; goals of care; irremediability; palliative psychiatry; quality of life; suffering.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Figures
References
-
- Beauchamp TL, Childress JF. (2019) Principles of Biomedical Ethics. Oxford: Oxford University Press.
-
- Berk M, Berk L, Udina M, et al.. (2012) Palliative models of care for later stages of mental disorder: Maximizing recovery, maintaining hope, and building morale. Australian and New Zealand Journal of Psychiatry 46: 92–99. - PubMed
-
- Bianchi A, Stanley K, Sutandar K. (2021) The ethical defensibility of harm reduction and eating disorders. The American Journal of Bioethics 21: 46–56. - PubMed
-
- Chochinov HM, Breitbart W. (2009) Handbook of Psychiatry in Palliative Medicine. New York: Oxford University Press.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
