

Case Reports
doi: 10.1002/ccr3.6263.
eCollection 2022 Aug.
Spinal Paget's disease with bilevel cord compression and ischemic non-compressive myelopathy treated with zoledronic acid
Affiliations
- PMID: 35999985
- PMCID: PMC9388838
- DOI: 10.1002/ccr3.6263
Item in Clipboard
Case Reports
Spinal Paget's disease with bilevel cord compression and ischemic non-compressive myelopathy treated with zoledronic acid
Clin Case Rep.
.
Abstract
Cord compression and ischemic non-compressive myelopathy are a complication of spinal Paget's disease (SPD). SPD usually touches a single spine level. We report an unusual case with bilevel spinal cord compression and dysfunction which was medically treated due to resolution of the vascular steal syndrome.
Keywords: Paget's bone disease; osteitis deformans; spinal cord compression; spine; zoledronic acid.
© 2022 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
None.
Figures
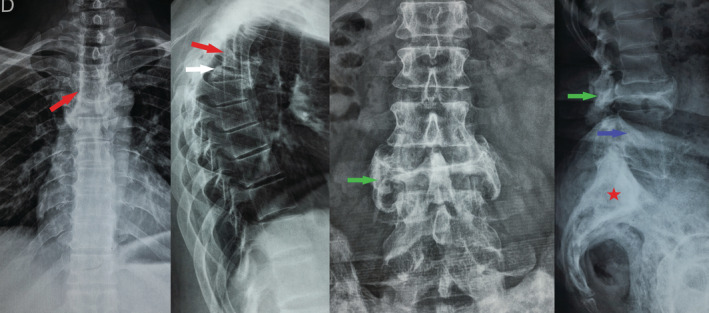
Thoracolumbar spine radiography showed thoracic spine deformation with bone heterogeneity, hypertrophy, and pathologic fracture of T4 (red arrow), T5 (white arrow), and L3 (green arrow). Vertebral ankylosis of L4/L5 (blue arrow) and heterogeneous architecture of the sacrum (red Asterix) were noted.

Chest and abdomen computed tomography objective left paravertebral mass extending to the area over the left trapezius. The density of the mass was equal to that of subcutaneous adipose tissue suggesting the diagnosis of typical simple lipoma.

Bone window of computed tomography with sagittal (A) and coronal (B) reconstructions of the spine and the pelvis showing pathologic fracture of T4 (red arrow), T5 (white arrow), and L3 (green arrow). There were lytic lesions of the vertebral body of T4 and the cortical of its inferior endplate with posterior elements involvement and local medullar cord compression at T5 and L3 levels. Vertebral ankylosis of L4/L5 (blue arrow) and heterogeneous architecture of the pelvis (red Asterix) were noted.

MRI of the spine. Abnormal pathological process of marrow infiltration and replacement involving T4, T5 (red arrow), and L3 (blue arrow) and their posterior neural arches (green Asterix), appearing as low signal on T1 (A) and high signal on T2‐weighted images (B), with non‐homogeneous enhancement (C). There was an expansion of the vertebral body and posterior elements of T4, T5, and L3. The asymmetric collapse of the T5 and L3 vertebra is noted with posterior vertebral surface convexity responsible for significant cord compression.

Whole‐body bone scintigraphy showing high osteoblastic activity in the spine, pelvis, and the left calcaneum (as marked with red arrows)
References
-
- Britton C, Walsh J. Paget disease of bone‐an update. Aust Fam Physician. 2012;41:100‐103. - PubMed
-
- Saifuddin A, Hassan A. Paget's disease of the spine: unusual features and complications. Clin Radiol. 2003;58:102‐111. - PubMed
-
- Bolland MJ, Cundy T. Paget's disease of bone: clinical review and update. J Clin Pathol. 2013;66:924‐927. - PubMed
-
- Vallet M, Ralston SH. Biology and treatment of Paget's disease of Bone. J Cell Biochem. 2016;117:289‐299. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
