

Quantification and visualization of aerosols in ear, nose, and throat exam and flexible laryngoscopy
- PMID: 36000064
- PMCID: PMC9392400
- DOI: 10.1002/lio2.826
Quantification and visualization of aerosols in ear, nose, and throat exam and flexible laryngoscopy
Abstract
Objective: To measure and visualize aerosol generation during ear, nose, and throat (ENT) exam and flexible laryngoscopy, as safety recommendations are currently to defer routine and low-priority examinations.
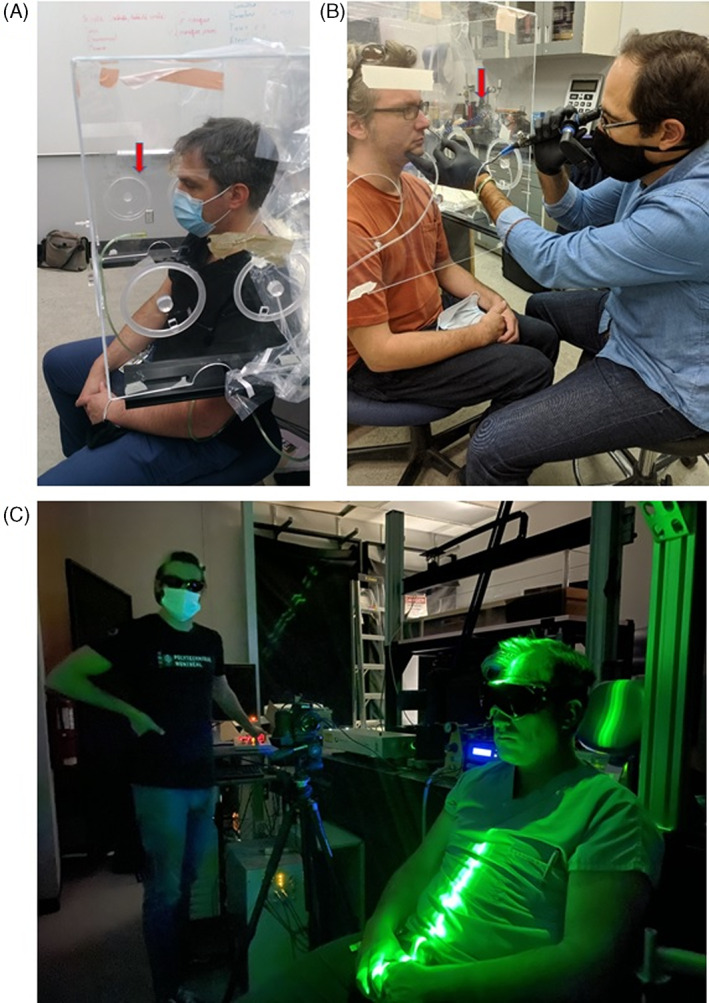
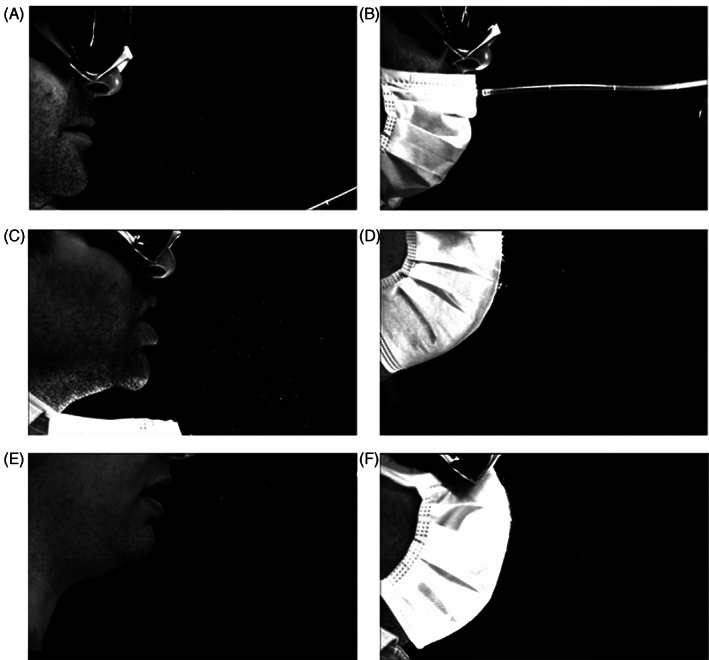
Methods: Aerosols generated during ENT examination and flexible laryngoscopy were quantified by laser aerosol spectrometry and visualized live by high-speed imaging during those procedures for three participants who were tested three times for each test.
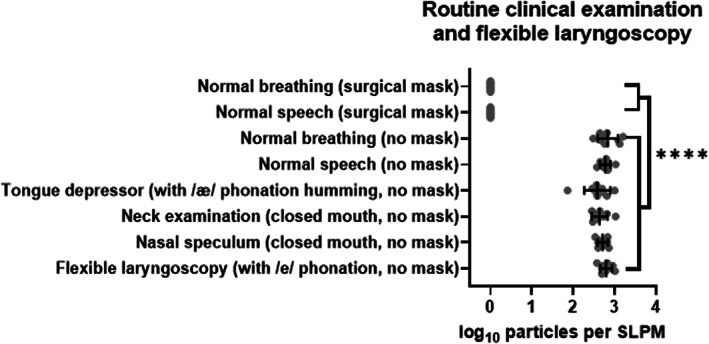
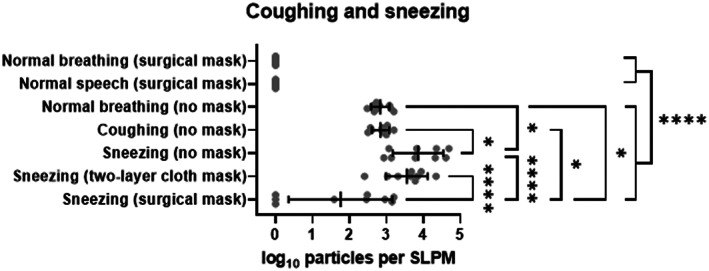
Results: Routine ENT examination and flexible laryngoscopy produce aerosols at levels comparable to normal breathing and speech.
Conclusion: During ENT examination and flexible laryngoscopy, the practitioner should wear a surgical mask and potentially contaminated surfaces should be cleaned after the procedure. For flexible laryngoscopy, it is recommended in addition that the patient wear a mask over the mouth in case the procedure induces a sneeze. The time during which the patient is unmasked should be minimized. In these settings, the risk to the practitioner is minimal unless the patient is sneezing or symptomatic.
Level of evidence: 1.
Keywords: COVID‐19; ENT examination; aerosols; flexible laryngoscopy; safety.
© 2022 The Authors. Laryngoscope Investigative Otolaryngology published by Wiley Periodicals LLC on behalf of The Triological Society.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Is Office Laryngoscopy an Aerosol-Generating Procedure?Laryngoscope. 2020 Nov;130(11):2637-2642. doi: 10.1002/lary.28973. Epub 2020 Jul 29. Laryngoscope. 2020. PMID: 32671840 Free PMC article.
-
Airborne Aerosol Generation During Endonasal Procedures in the Era of COVID-19: Risks and Recommendations.Otolaryngol Head Neck Surg. 2020 Sep;163(3):465-470. doi: 10.1177/0194599820931805. Epub 2020 May 26. Otolaryngol Head Neck Surg. 2020. PMID: 32452739 Free PMC article.
-
Evaluating a Prototype Nasolaryngoscopy Hood During Aerosol-Generating Procedures in Otolaryngology.Otolaryngol Head Neck Surg. 2021 Jun;164(6):1251-1256. doi: 10.1177/0194599820973652. Epub 2020 Nov 24. Otolaryngol Head Neck Surg. 2021. PMID: 33228434 Free PMC article.
-
Seven cardinal questions for the patient with ear, nose or throat complaints: Review.Medicine (Baltimore). 2022 Dec 16;101(50):e31852. doi: 10.1097/MD.0000000000031852. Medicine (Baltimore). 2022. PMID: 36550869 Free PMC article. Review.
-
Ear, Nose, and Throat Practice Guidelines: An Update for COVID-19.Int Arch Otorhinolaryngol. 2021 Aug 4;25(4):e621-e627. doi: 10.1055/s-0041-1736424. eCollection 2021 Oct. Int Arch Otorhinolaryngol. 2021. PMID: 34777595 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous