

Identifying Potentially Unnecessary Hospitalizations in Children With Pneumonia
- PMID: 36000331
- PMCID: PMC11315224
- DOI: 10.1542/hpeds.2022-006608
Identifying Potentially Unnecessary Hospitalizations in Children With Pneumonia
Abstract
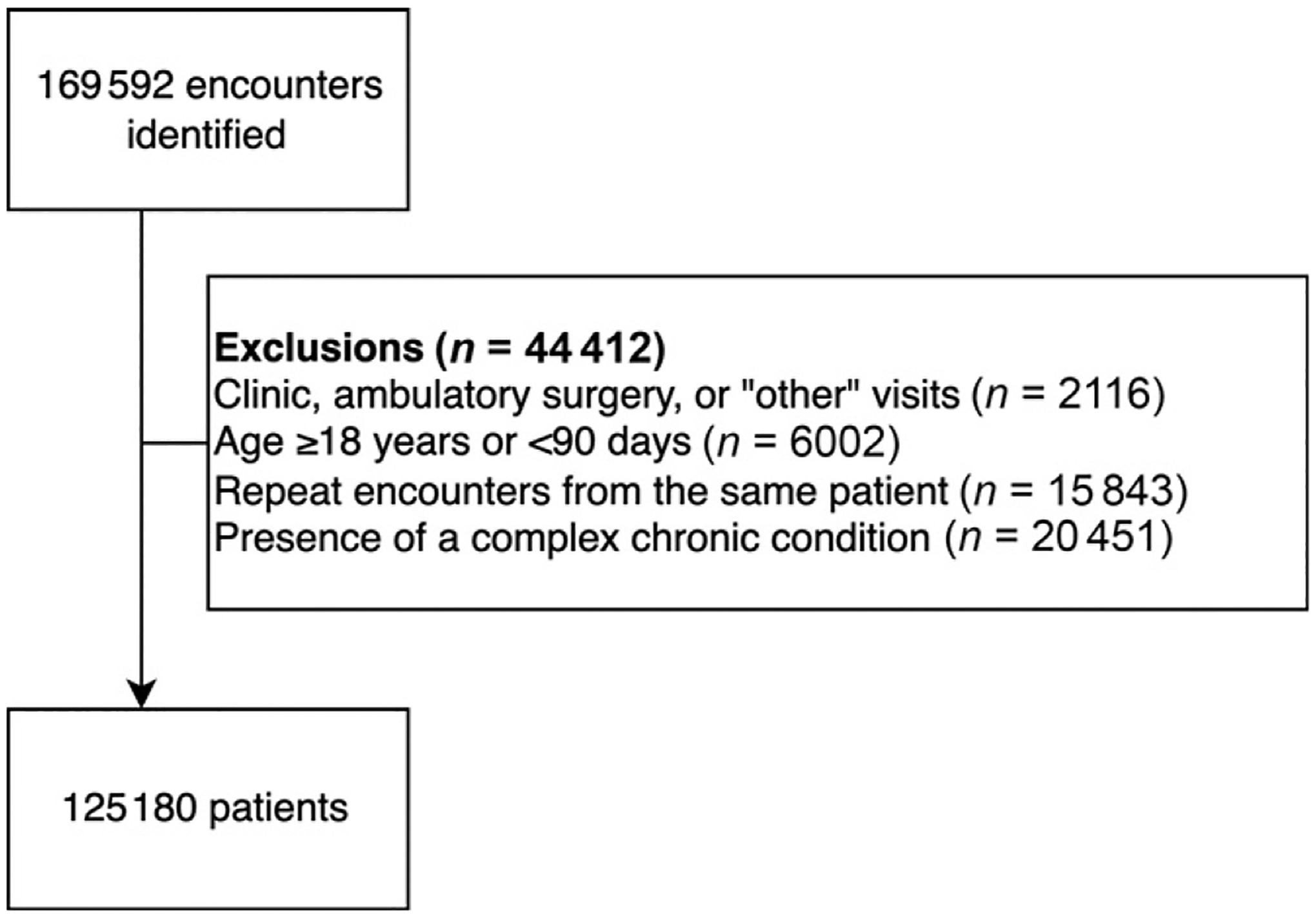
Objective: To characterize the outcomes of children with community acquired pneumonia (CAP) across 41 United States hospitals and evaluate factors associated with potentially unnecessary admissions.
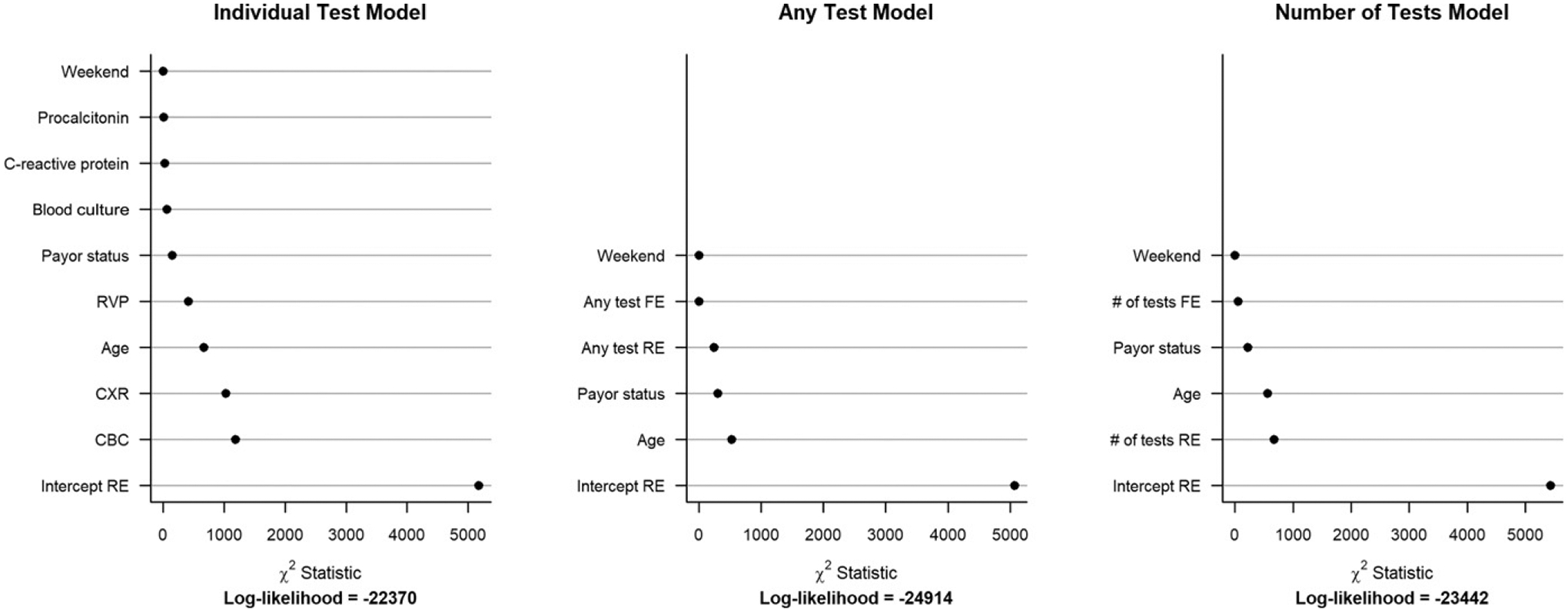
Methods: We performed a cross-sectional study of patients with CAP from 41 United States pediatric hospitals and evaluated clinical outcomes using a composite ordinal severity outcome: mild-discharged (discharged from the emergency department), mild-admitted (hospitalized without other interventions), moderate (provision of intravenous fluids, supplemental oxygen, broadening of antibiotics, complicated pneumonia, and presumed sepsis) or severe (ICU, positive-pressure ventilation, vasoactive infusion, chest drainage, extracorporeal membrane oxygenation, severe sepsis, or death). Our primary outcome was potentially unnecessary admissions (ie, mild-admitted). Among mild-discharged and mild-admitted patients, we constructed a generalized linear mixed model for mild-admitted severity and assessed the role of fixed (demographics and clinical testing) and random effects (institution) on this outcome.
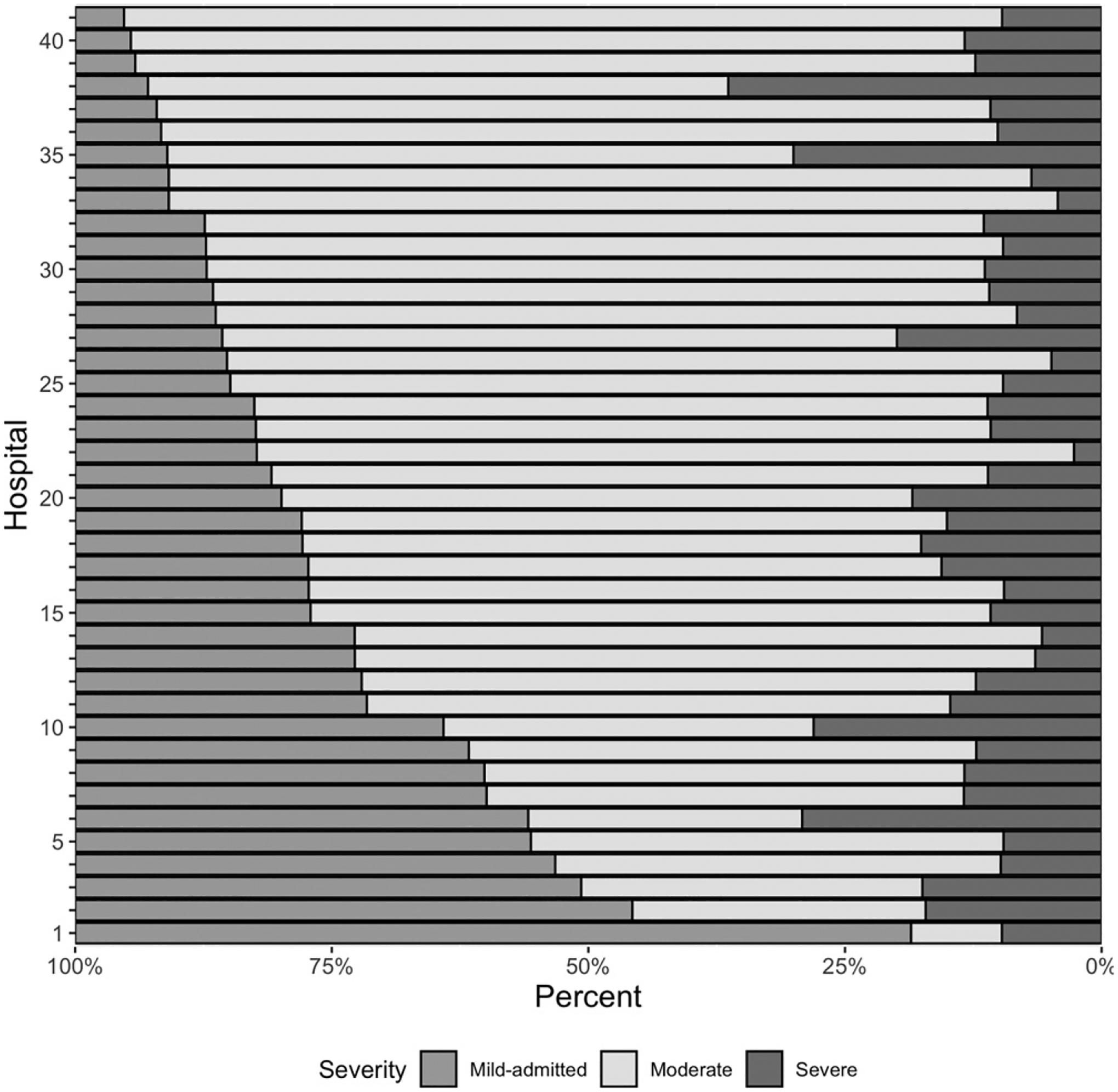
Results: Of 125 180 children, 68.3% were classified as mild-discharged, 6.6% as mild-admitted, 20.6% as moderate and 4.5% as severe. Among admitted patients (n = 39 692), 8321 (21%) were in the mild-admitted group, with substantial variability in this group across hospitals (median 19.1%, interquartile range 12.8%-28.4%). In generalized linear mixed models comparing mild-admitted and mild-discharge severity groups, hospital had the greatest contribution to model variability compared to all other variables.
Conclusions: One in 5 hospitalized children with CAP do not receive significant interventions. Among patients with mild disease, institutional variation is the most important contributor to predict potentially unnecessary admissions. Improved prognostic tools are needed to reduce potentially unnecessary hospitalization of children with CAP.
Copyright © 2022 by the American Academy of Pediatrics.
Conflict of interest statement
Figures
References
-
- Harris M, Clark J, Coote N, et al. ; British Thoracic Society Standards of Care Committee. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax. 2011;66(Suppl 2):ii1–ii23 - PubMed
-
- Keren R, Luan X, Localio R, et al. ; Pediatric Research in Inpatient Settings (PRIS) Network. Prioritization of comparative effectiveness research topics in hospital pediatrics. Arch Pediatr Adolesc Med. 2012;166(12): 1155–1164 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
