

Gut Microbiota and Coronary Plaque Characteristics
- PMID: 36000423
- PMCID: PMC9496418
- DOI: 10.1161/JAHA.122.026036
Gut Microbiota and Coronary Plaque Characteristics
Abstract
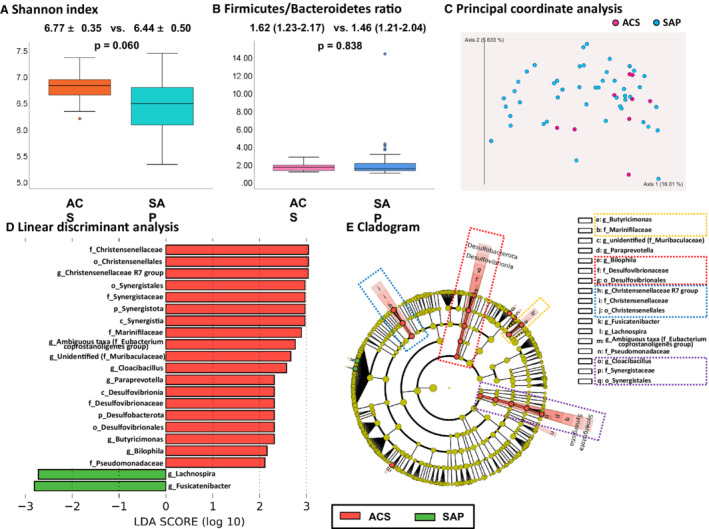
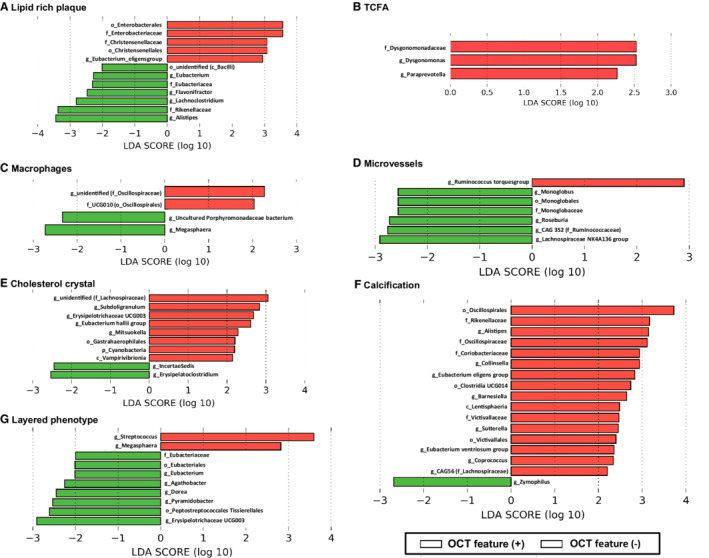
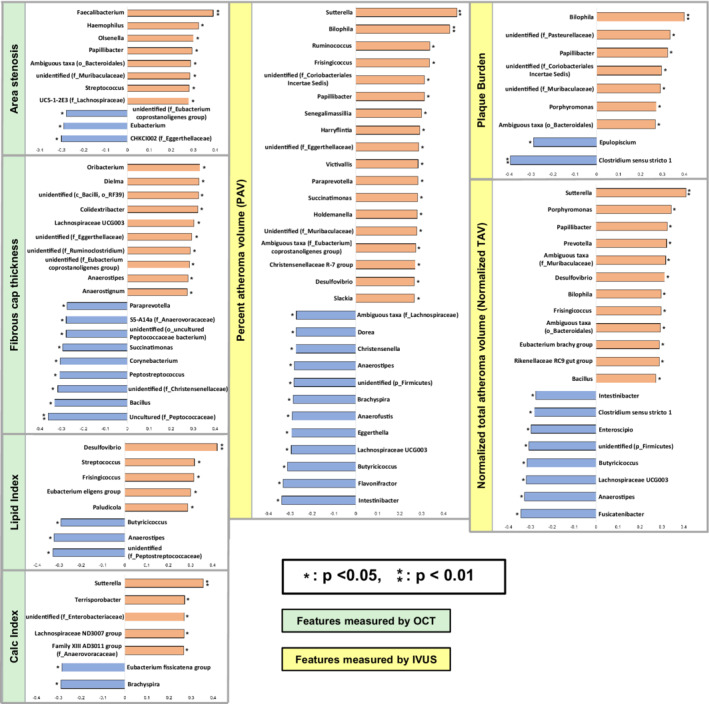
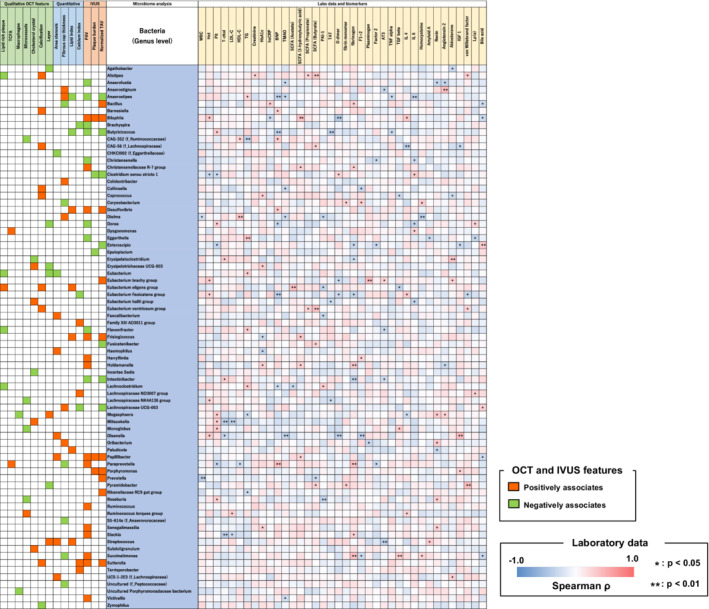
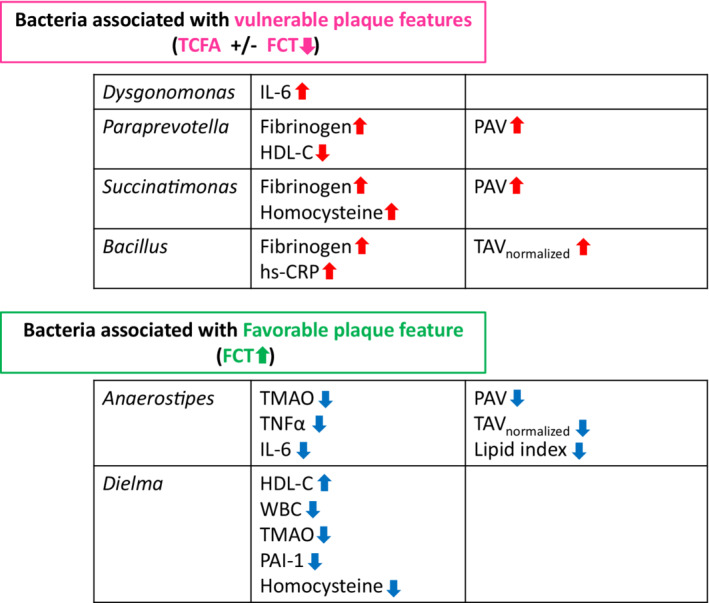
Background The relationship between gut microbiota and in vivo coronary plaque characteristics has not been reported. This study was conducted to investigate the relationship between gut microbiota and coronary plaque characteristics in patients with coronary artery disease. Methods and Results Patients who underwent both optical coherence tomography and intravascular ultrasound imaging and provided stool and blood specimens were included. The composition of gut microbiota was evaluated using 16S rRNA sequencing. A total of 55 patients were included. At the genus level, 2 bacteria were associated with the presence of thin-cap fibroatheroma, and 9 bacteria were associated with smaller fibrous cap thickness. Among them, some bacteria had significant associations with inflammatory/prothrombotic biomarkers. Dysgonomonas had a positive correlation with interleukin-6, Paraprevotella had a positive correlation with fibrinogen and negative correlation with high-density lipoprotein cholesterol, Succinatimonas had positive correlations with fibrinogen and homocysteine, and Bacillus had positive correlations with fibrinogen and high-sensitivity C-reactive protein. In addition, Paraprevotella, Succinatimonas, and Bacillus were also associated with greater plaque volume. Ten bacteria were associated with larger fibrous cap thickness. Some were associated with protective biomarker changes; Anaerostipes had negative correlations with trimethylamine N-oxide, tumor necrosis factor α, and interleukin-6, and Dielma had negative correlations with trimethylamine N-oxide, white blood cells, plasminogen activator inhibitor-1, and homocysteine, and a positive correlation with high-density lipoprotein cholesterol. Conclusions Bacteria that were associated with vulnerable coronary plaque phenotype and greater plaque burden were identified. These bacteria were also associated with elevated inflammatory or prothrombotic biomarkers. Registration URL: https://www.umin.ac.jp/ctr/; Unique identifier: UMIN000041692.
Keywords: 16S rRNA; biomarkers; coronary artery disease; gut microbiota; intravascular ultrasound; optical coherence tomography; vulnerable plaque.
Figures
References
-
- Verhaar BJH, Collard D, Prodan A, Levels JHM, Zwinderman AH, Backhed F, Vogt L, Peters MJL, Muller M, Nieuwdorp M, et al. Associations between gut microbiota, faecal short‐chain fatty acids, and blood pressure across ethnic groups: the HELIUS study. Eur Heart J. 2020;41:4259–4267. doi: 10.1093/eurheartj/ehaa704 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
