

Renin-Angiotensin System Inhibitors in Patients With COVID-19: A Meta-Analysis of Randomized Controlled Trials Led by the International Society of Hypertension
- PMID: 36000426
- PMCID: PMC9496439
- DOI: 10.1161/JAHA.122.026143
Renin-Angiotensin System Inhibitors in Patients With COVID-19: A Meta-Analysis of Randomized Controlled Trials Led by the International Society of Hypertension
Abstract
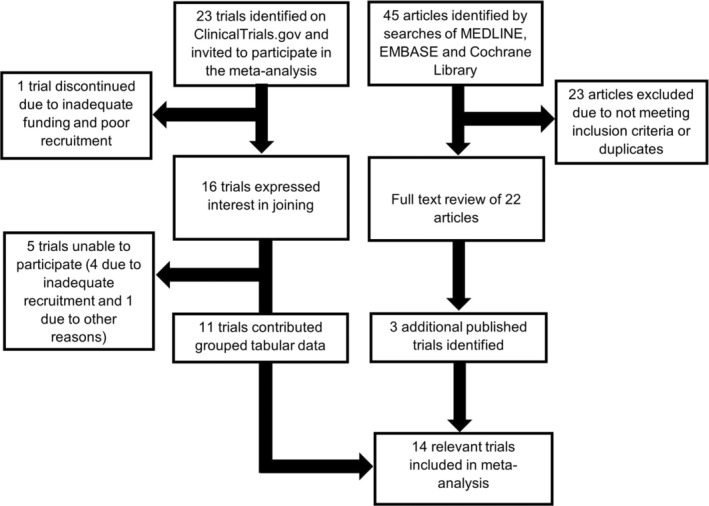
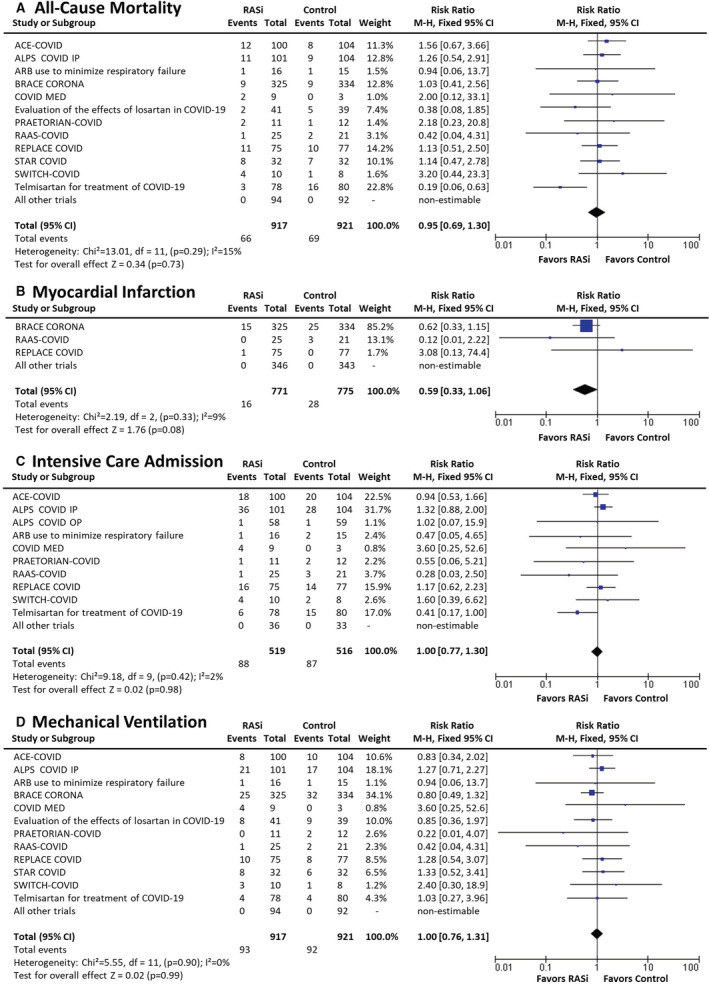
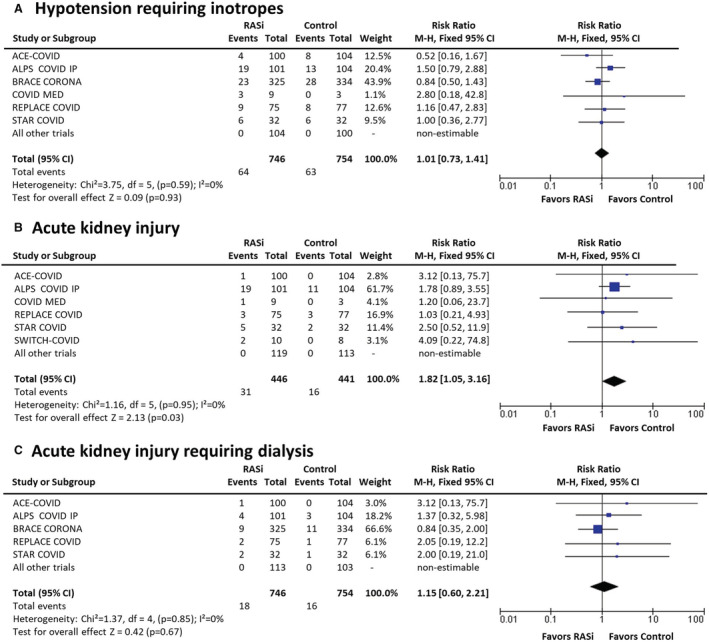
Background Published randomized controlled trials are underpowered for binary clinical end points to assess the safety and efficacy of renin-angiotensin system inhibitors (RASi) in adults with COVID-19. We therefore performed a meta-analysis to assess the safety and efficacy of RASi in adults with COVID-19. Methods and Results MEDLINE, EMBASE, ClinicalTrials.gov, and the Cochrane Controlled Trial Register were searched for randomized controlled trials that randomly assigned patients with COVID-19 to RASi continuation/commencement versus no RASi therapy. The primary outcome was all-cause mortality at ≤30 days. A total of 14 randomized controlled trials met the inclusion criteria and enrolled 1838 participants (aged 59 years, 58% men, mean follow-up 26 days). Of the trials, 11 contributed data. We found no effect of RASi versus control on all-cause mortality (7.2% versus 7.5%; relative risk [RR], 0.95; [95% CI, 0.69-1.30]) either overall or in subgroups defined by COVID-19 severity or trial type. Network meta-analysis identified no difference between angiotensin-converting enzyme inhibitors versus angiotensin II receptor blockers. RASi users had a nonsignificant reduction in acute myocardial infarction (2.1% versus 3.6%; RR, 0.59; [95% CI, 0.33-1.06]), but increased risk of acute kidney injury (7.0% versus 3.6%; RR, 1.82; [95% CI, 1.05-3.16]), in trials that initiated and continued RASi. There was no increase in need for dialysis or differences in congestive cardiac failure, cerebrovascular events, venous thromboembolism, hospitalization, intensive care admission, inotropes, or mechanical ventilation. Conclusions This meta-analysis of randomized controlled trials evaluating angiotensin-converting enzyme inhibitors/angiotensin II receptor blockers versus control in patients with COVID-19 found no difference in all-cause mortality, a borderline decrease in myocardial infarction, and an increased risk of acute kidney injury with RASi. Our findings provide strong evidence that RASi can be used safely in patients with COVID-19.
Keywords: COVID‐19; acute kidney injury; angiotensin II receptor blockers; angiotensin‐converting enzyme inhibitors; hypertension; renin‐angiotensin system inhibitors.
Figures
References
-
- Gu Q, Burt VL, Dillon CF, Yoon S. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension: the National Health And Nutrition Examination Survey, 2001 to 2010. Circulation. 2012;126:2105–2114. doi: 10.1161/CIRCULATIONAHA.112.096156 - DOI - PubMed
-
- Ferrario CM, Jessup J, Chappell MC, Averill DB, Brosnihan KB, Tallant EA, Diz DI, Gallagher PE. Effect of angiotensin‐converting enzyme inhibition and angiotensin II receptor blockers on cardiac angiotensin‐converting enzyme 2. Circulation. 2005;111:2605–2610. doi: 10.1161/CIRCULATIONAHA.104.510461 - DOI - PubMed
-
- Ocaranza MP, Moya J, Barrientos V, Alzamora R, Hevia D, Morales C, Pinto M, Escudero N, García L, Novoa U, et al. Angiotensin‐(1‐9) reverses experimental hypertension and cardiovascular damage by inhibition of the angiotensin converting enzyme/Ang II axis. J Hypertens. 2014;32:771–783. doi: 10.1097/HJH.0000000000000094 - DOI - PubMed
-
- Hoffmann M, Kleine‐Weber H, Schroeder S, Krüger N, Herrler T, Erichsen S, Schiergens TS, Herrler G, Wu NH, Nitsche A, et al. SARS‐CoV‐2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181:271–280.e8. doi: 10.1016/j.cell.2020.02.052 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
