

Longitudinal clinical study of patients with iron rim lesions in multiple sclerosis
- PMID: 36000485
- PMCID: PMC9679801
- DOI: 10.1177/13524585221114750
Longitudinal clinical study of patients with iron rim lesions in multiple sclerosis
Abstract
Background: Iron rims (IRs) surrounding white matter lesions (WMLs) are suggested to predict a more severe disease course. Only small longitudinal cohorts of patients with and without iron rim lesions (IRLs) have been reported so far.
Objective: To assess whether the presence and number of IRLs in patients with clinically isolated syndrome (CIS) and multiple sclerosis (MS) are associated with long-term disability or progressive disease.
Methods: Ninety-one CIS/MS patients were recruited between 2008 and 2013 and scanned with 7 T magnetic resonance imaging (MRI). Expanded Disability Status Scale (EDSS) was used to calculate Age-related Multiple Sclerosis Severity Score (ARMSS) at the time of scan and at the latest clinical follow-up after 9 years. WMLs were assessed for the presence of IRL using Susceptibility weighted imaging (SWI)-filtered phase images.
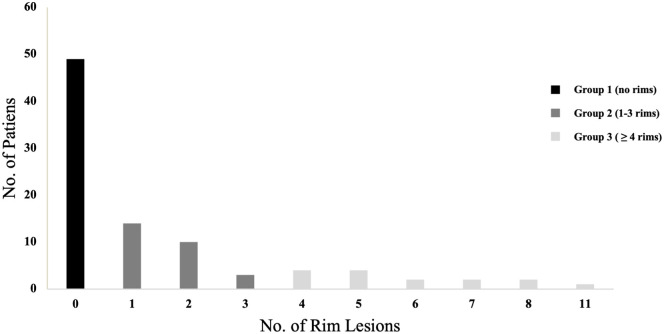
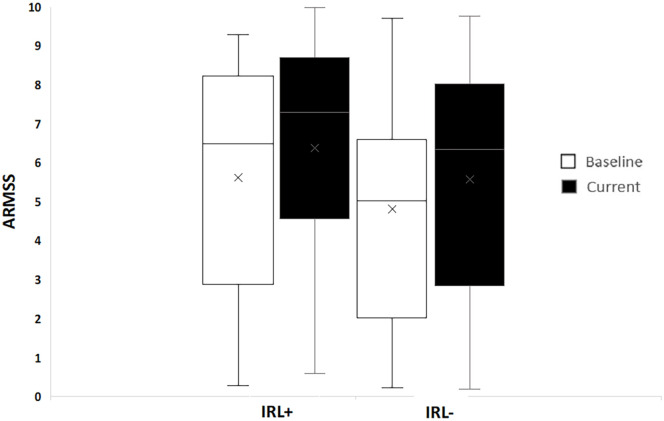
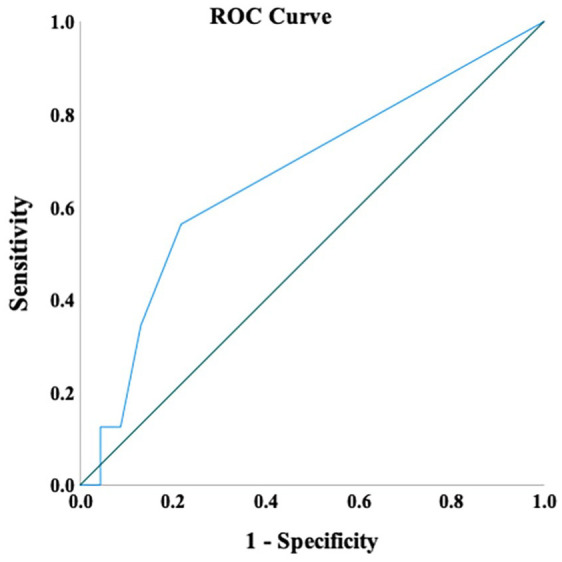
Results: In all, 132 IRLs were detected in 42 patients (46%); 9% of WMLs had IRs; 54% of the cohort had no rims, 30% had 1-3 rims and 16% had ⩾4. Patients with IRL had a higher EDSS and ARMSS. Presence of IRL was also a predictor of long-term disability, especially in patients with ⩾4 IRLs. IRLs have a greater impact on disability compared to the WML number and volume.
Conclusion: The presence and number of perilesional IR on MRI hold prognostic value for long-term clinical disability in MS.
Keywords: Multiple sclerosis (MS); biomarkers; iron rim lesion (IRL); magnetic resonance imaging (MRI); white matter lesion (WML).
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: A.I.A., A.M.H, A.A., S.-Y.L. and O.M. have nothing to declare. C.M.A. has received speaker honorarium from the Multiple Sclerosis Academy. R.A.-F. has participated on advisory boards, received travel grants and attended educational programmes sponsored by Roche and Novartis. C.S.C. has received grants, personal fees and nonfinancial support from Biogen; and personal fees and nonfinancial support from Novartis, Teva, Merck and Sanofi Genzyme. N.E. is a member of the advisory board for Biogen, Merck, Novartis and Roche; he has received grant income from the MS Society, MRC, PCORI and NIHR.
Figures



References
-
- Rosati G. The prevalence of multiple sclerosis in the world: An update. Neurol Sci 2001; 22(2): 117–139. - PubMed
-
- Ontaneda D, Tallantyre E, Kalincik T, et al.. Early highly effective versus escalation treatment approaches in relapsing multiple sclerosis. Lancet Neurol 2019; 18(10): 973–980. - PubMed
-
- Rotstein D, Montalban X. Reaching an evidence-based prognosis for personalized treatment of multiple sclerosis. Nat Rev Neurol 2019; 15(5): 287–300. - PubMed
-
- Allen CM, Mowry E, Tintore M, et al.. Prognostication and contemporary management of clinically isolated syndrome. J Neurol Neurosurg Psychiatry 2021; 92(4): 391–397. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
