

Assessing splenic switch-off in Adenosine stress CMR for patients with atrial fibrillation: a propensity-matched study
- PMID: 36000672
- PMCID: PMC9793484
- DOI: 10.1259/bjr.20220422
Assessing splenic switch-off in Adenosine stress CMR for patients with atrial fibrillation: a propensity-matched study
Abstract
Objectives: Splenic switch-off (SSO) is a validated indicator of adequate vasodilator stress unique to adenosine stress cardiac MR (CMR). Patients in atrial fibrillation (AF) may have a reduced adenosine response due to lower hyperaemic coronary flow reserve and may achieve SSO less frequently versus sinus rhythm (SR).
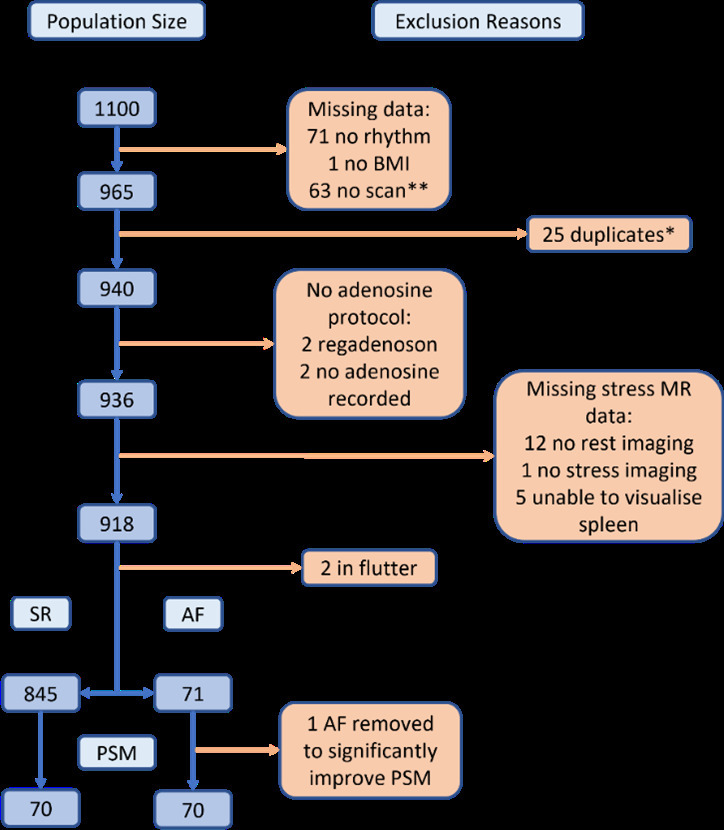
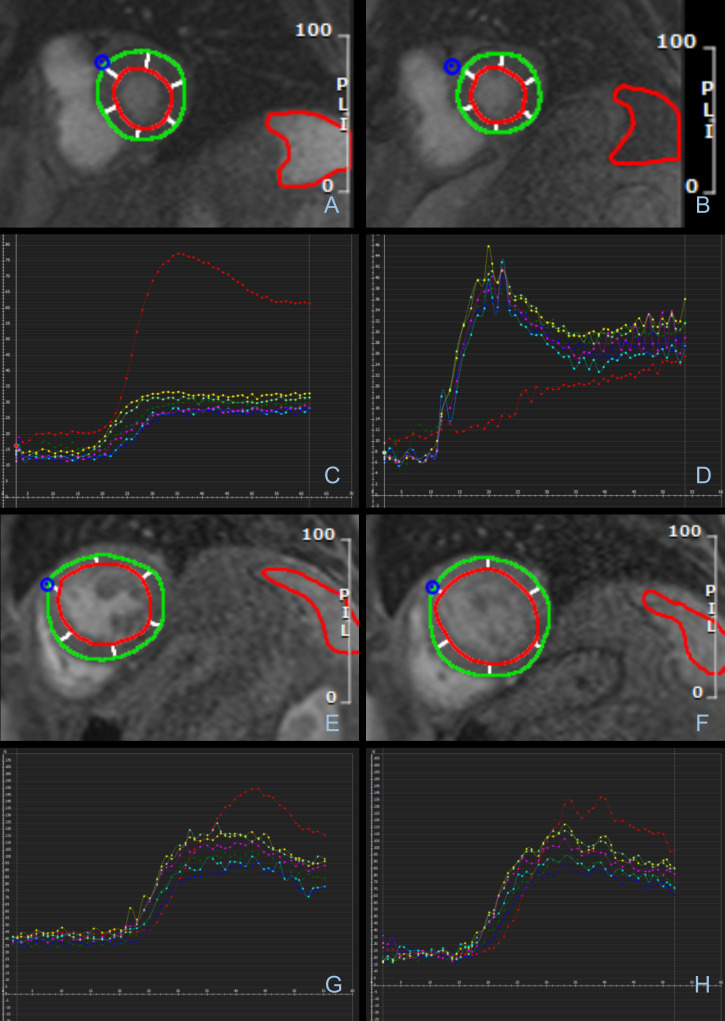
Methods: 1100 stress CMR studies were identified from a clinical CMR database (2016-2021). 70 patients in AF were propensity score matched to a SR group for age, sex, and body mass index. The adenosine dose administered, symptoms, heart-rate change and scan result were recorded. SSO was evaluated subjectively and semi-quantitatively via changes in splenic and myocardial signal intensity (SI) from rest to stress.
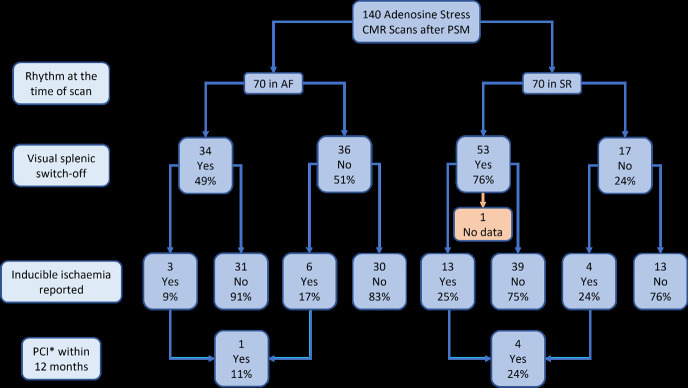
Results: SSO occurred significantly less frequently in AF than SR (34/70 [49%] vs 53/70 [76%], p = 0.003). Semi-quantitative assessment supported this, with a smaller splenic SI difference between stress and rest in AF vs SR (median splenic stress:rest peak SI ratio 0.92 [IQR:0.61-1.11] vs 0.56 [IQR:0.45-0.75], p < 0.001). A heart-rate increase >10 bpm predicted visual SSO in SR but not AF. Fewer patients in AF than SR had inducible ischaemia (9/70 [13%] vs 17/69 [25%], p = 0.058). This difference was not driven by inducible ischaemia rates in patients who did not achieve SSO (6/36 [17%] AF vs 4/17 [24%] SR, p = 0.403).
Conclusions: SSO occurs significantly less frequently with AF. This may risk the under diagnosis of inducible ischaemia and requires further assessment.
Advances in knowledge: SSO, a validated marker of adequate stress in CMR, occurs significantly less frequently in the presence of AF, risking a suboptimal functional assessment of coronary disease.
Conflict of interest statement
Figures
Similar articles
-
Haemodynamic and hyperaemic effects of adenosine in patients with atrial fibrillation undergoing quantitative myocardial perfusion cardiovascular magnetic resonance.Eur Heart J Imaging Methods Pract. 2024 Dec 26;2(3):qyae127. doi: 10.1093/ehjimp/qyae127. eCollection 2024 Jul. Eur Heart J Imaging Methods Pract. 2024. PMID: 39726566 Free PMC article.
-
Splenic switch-off as a novel marker for adenosine response in nitrogen-13 ammonia PET myocardial perfusion imaging: Cross-validation against CMR using a hybrid PET/MR device.J Nucl Cardiol. 2022 Jun;29(3):1205-1214. doi: 10.1007/s12350-020-02448-y. Epub 2020 Dec 22. J Nucl Cardiol. 2022. PMID: 33354759 Free PMC article.
-
Splenic switch-off as a predictor for coronary adenosine response: validation against 13N-ammonia during co-injection myocardial perfusion imaging on a hybrid PET/CMR scanner.J Cardiovasc Magn Reson. 2021 Jan 7;23(1):3. doi: 10.1186/s12968-020-00696-y. J Cardiovasc Magn Reson. 2021. PMID: 33407586 Free PMC article.
-
Splenic Switch-Off for Determining the Optimal Dosage for Adenosine Stress Cardiac MR in Terms of Stress Effectiveness and Patient Safety.J Magn Reson Imaging. 2020 Dec;52(6):1732-1742. doi: 10.1002/jmri.27248. Epub 2020 Jun 18. J Magn Reson Imaging. 2020. PMID: 32557923 Clinical Trial.
-
Disagreement between splenic switch-off and myocardial T1-mapping after caffeine intake.Int J Cardiovasc Imaging. 2018 Apr;34(4):625-632. doi: 10.1007/s10554-017-1274-0. Epub 2017 Nov 24. Int J Cardiovasc Imaging. 2018. PMID: 29177579 Free PMC article.
Cited by
-
Haemodynamic and hyperaemic effects of adenosine in patients with atrial fibrillation undergoing quantitative myocardial perfusion cardiovascular magnetic resonance.Eur Heart J Imaging Methods Pract. 2024 Dec 26;2(3):qyae127. doi: 10.1093/ehjimp/qyae127. eCollection 2024 Jul. Eur Heart J Imaging Methods Pract. 2024. PMID: 39726566 Free PMC article.
References
-
- Recent-onset chest pain of suspected cardiac origin: assessment and diagnosis. London: National Institute for Health and. 2016. Available from: https://www.nice.org.uk/guidance/cg95/chapter/Recommendations - PubMed
-
- Greenwood JP, Ripley DP, Berry C, McCann GP, Plein S, Bucciarelli-Ducci C, et al. . CE-MARC 2 Investigators. In: Effect of Care Guided by Cardiovascular Magnetic Resonance, Myocardial Perfusion Scintigraphy, or NICE Guidelines on Subsequent Unnecessary Angiography Rates: The CE-MARC 2 Randomized Clinical Trial. JAMA. ; September 2016., pp. 1051–60. doi: 10.1001/jama.2016.12680 - DOI - PubMed
-
- Einstein A, Fisher D, Gregory S, Hansen C, Messana S. Pharmacologic and Exercise Stress Tests. 2011. Available from: https://www.asnc.org/practicepoints
-
- Brown LAE, Saunderson CED, Das A, Craven T, Levelt E, Knott KD, et al. . A comparison of standard and high dose adenosine protocols in routine vasodilator stress cardiovascular magnetic resonance: dosage affects hyperaemic myocardial blood flow in patients with severe left ventricular systolic impairment. J Cardiovasc Magn Reson 2021; 23: 37. doi: 10.1186/s12968-021-00714-7 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
