

Systematic review and meta-analysis comparing low-flow duration of extracorporeal and conventional cardiopulmonary resuscitation
- PMID: 36000900
- PMCID: PMC9491846
- DOI: 10.1093/icvts/ivac219
Systematic review and meta-analysis comparing low-flow duration of extracorporeal and conventional cardiopulmonary resuscitation
Abstract
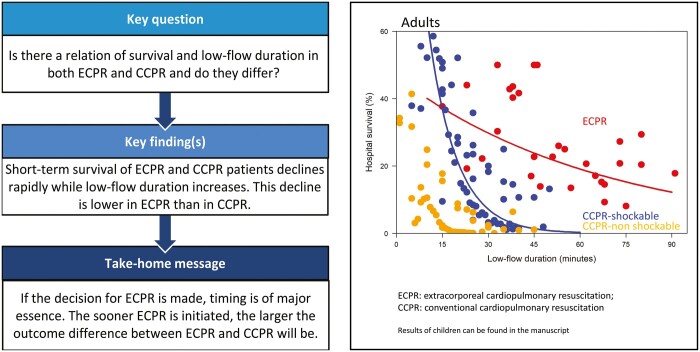
Objectives: After cardiac arrest, a key factor determining survival outcomes is low-flow duration. Our aims were to determine the relation of survival and low-flow duration of extracorporeal cardiopulmonary resuscitation (ECPR) and conventional cardiopulmonary resuscitation (CCPR) and if these 2 therapies have different short-term survival curves in relation to low-flow duration.
Methods: We searched Embase, Medline, Web of Science and Google Scholar from inception up to April 2021. A linear mixed-effect model was used to describe the course of survival over time, based on study-specific and time-specific aggregated survival data.
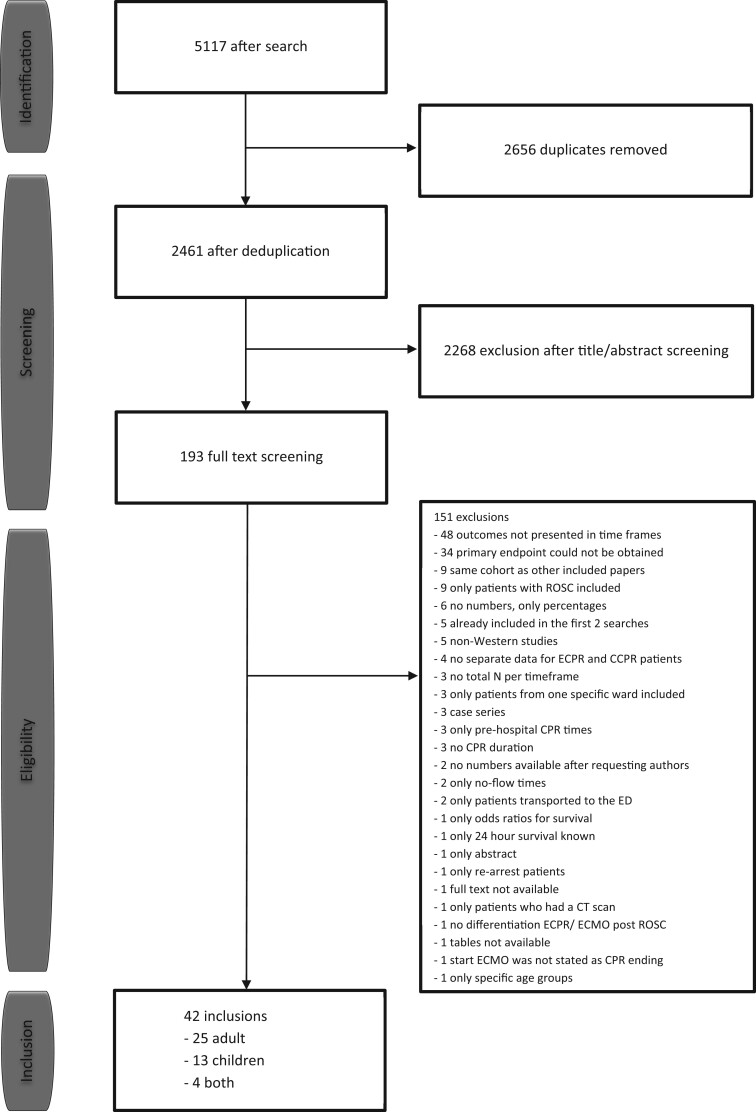
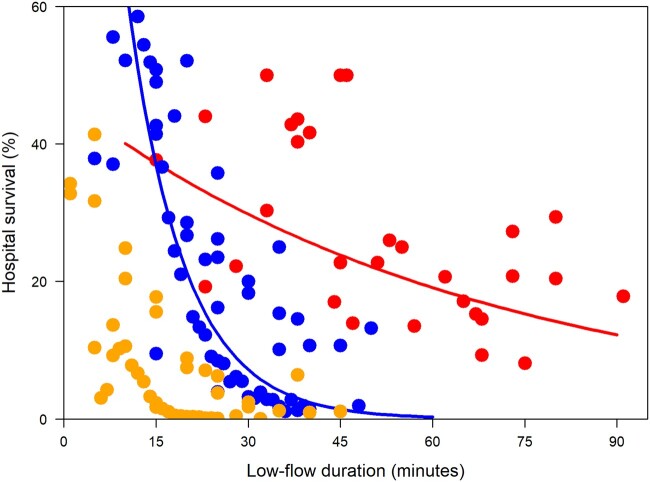
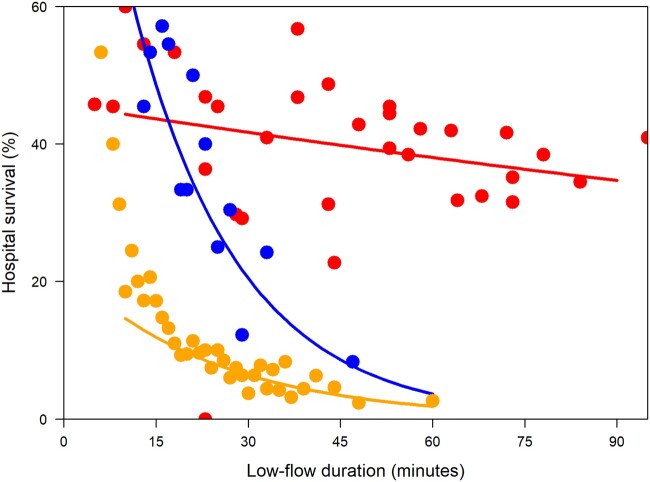
Results: We included 42 observational studies reporting on 1689 ECPR and 375 751 CCPR procedures. Of the included studies, 25 included adults, 13 included children and 4 included both. In adults, survival curves decline rapidly over time (ECPR 37.2%, 29.8%, 23.8% and 19.1% versus CCPR-shockable 36.8%, 7.2%, 1.4% and 0.3% for 15, 30, 45 and 60 min low-flow, respectively). ECPR was associated with a statistically significant slower decline in survival than CCPR with initial shockable rhythms (CCPR-shockable). In children, survival curves decline rapidly over time (ECPR 43.6%, 41.7%, 39.8% and 38.0% versus CCPR-shockable 48.6%, 20.5%, 8.6% and 3.6% for 15, 30, 45 and 60 min low-flow, respectively). ECPR was associated with a statistically significant slower decline in survival than CCPR-shockable.
Conclusions: The short-term survival of ECPR and CCPR-shockable patients both decline rapidly over time, in adults as well as in children. This decline of short-term survival in relation to low-flow duration in ECPR was slower than in conventional cardiopulmonary resuscitation.
Trial registration: Prospero: CRD42020212480, 2 October 2020.
Keywords: Cardiac arrest; Cardiopulmonary resuscitation; Extracorporeal cardiopulmonary resuscitation; Heart arrest; Survival.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
Similar articles
-
Extracorporeal and Conventional Cardiopulmonary Resuscitation and Low-Flow Duration: Insights From a Nationwide Hospital-Based Registry Study in Japan (JAAM-OHCA Registry).J Am Heart Assoc. 2025 Jul 15;14(14):e039938. doi: 10.1161/JAHA.124.039938. Epub 2025 Jul 14. J Am Heart Assoc. 2025. PMID: 40654244
-
Comparing extracorporeal cardiopulmonary resuscitation with conventional cardiopulmonary resuscitation: A meta-analysis.Resuscitation. 2016 Jun;103:106-116. doi: 10.1016/j.resuscitation.2016.01.019. Epub 2016 Feb 2. Resuscitation. 2016. PMID: 26851058 Review.
-
Extracorporeal cardiopulmonary resuscitation versus conventional cardiopulmonary resuscitation in adults with cardiac arrest: a comparative meta-analysis and trial sequential analysis.Lancet Respir Med. 2023 Oct;11(10):883-893. doi: 10.1016/S2213-2600(23)00137-6. Epub 2023 May 22. Lancet Respir Med. 2023. PMID: 37230097
-
Long-term health-related quality of life in survivors of extracorporeal cardiopulmonary resuscitation compared to conventional cardiopulmonary resuscitation- A cohort study using Australian and New Zealand extracorporeal membrane oxygenation registry and the Victorian Ambulance Cardiac Arrest Registry.Resuscitation. 2025 May;210:110601. doi: 10.1016/j.resuscitation.2025.110601. Epub 2025 Apr 3. Resuscitation. 2025. PMID: 40187545
-
An optimal transition time to extracorporeal cardiopulmonary resuscitation for predicting good neurological outcome in patients with out-of-hospital cardiac arrest: a propensity-matched study.Crit Care. 2014 Sep 26;18(5):535. doi: 10.1186/s13054-014-0535-8. Crit Care. 2014. PMID: 25255842 Free PMC article.
Cited by
-
The impact of door to extracorporeal cardiopulmonary resuscitation time on mortality and neurological outcomes among out-of-hospital cardiac arrest acute myocardial infarction patients treated by primary percutaneous coronary intervention.Am Heart J Plus. 2024 Oct 14;47:100473. doi: 10.1016/j.ahjo.2024.100473. eCollection 2024 Nov. Am Heart J Plus. 2024. PMID: 39503005 Free PMC article.
-
First Results of Our Local Practice Guide Used During the Late Phase of Resuscitation in Patients with Refractory VF in Out of Hospital Cardiac Arrest.Open Access Emerg Med. 2025 May 28;17:203-213. doi: 10.2147/OAEM.S510483. eCollection 2025. Open Access Emerg Med. 2025. PMID: 40453369 Free PMC article.
-
A national multi centre pre-hospital ECPR stepped wedge study; design and rationale of the ON-SCENE study.Scand J Trauma Resusc Emerg Med. 2024 Apr 17;32(1):31. doi: 10.1186/s13049-024-01198-x. Scand J Trauma Resusc Emerg Med. 2024. PMID: 38632661 Free PMC article. Clinical Trial.
-
Favorable resuscitation characteristics in patients undergoing extracorporeal cardiopulmonary resuscitation: A secondary analysis of the INCEPTION-trial.Resusc Plus. 2024 May 13;18:100657. doi: 10.1016/j.resplu.2024.100657. eCollection 2024 Jun. Resusc Plus. 2024. PMID: 38778803 Free PMC article.
-
Differences in Treatment Outcomes According to the Insertion Method Used in Extracorporeal Cardiopulmonary Resuscitation: A Single-Center Experience.J Chest Surg. 2024 May 5;57(3):281-288. doi: 10.5090/jcs.23.118. Epub 2024 Mar 13. J Chest Surg. 2024. PMID: 38472119 Free PMC article.
References
-
- World Health Organisation. 2020. https://www.who.int/ (1 February 2020, date last accessed).
-
- Patz T, Stelzig K, Pfeifer R, Pittl U, Thiele H, Busch HJ. et al. Age-associated outcomes after survived out-of-hospital cardiac arrest and subsequent target temperature management. Acta Anaesthesiol Scand 2019;63:1079–88. - PubMed
-
- Zhang Q, Qi Z, Liu B, Li C.. Predictors of survival and favorable neurological outcome in patients treated with targeted temperature management after cardiac arrest: a systematic review and meta-analysis. Heart Lung 2018;47:602–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
