

Proteogenomic Markers of Chemotherapy Resistance and Response in Triple-Negative Breast Cancer
- PMID: 36001024
- PMCID: PMC9627136
- DOI: 10.1158/2159-8290.CD-22-0200
Proteogenomic Markers of Chemotherapy Resistance and Response in Triple-Negative Breast Cancer
Abstract
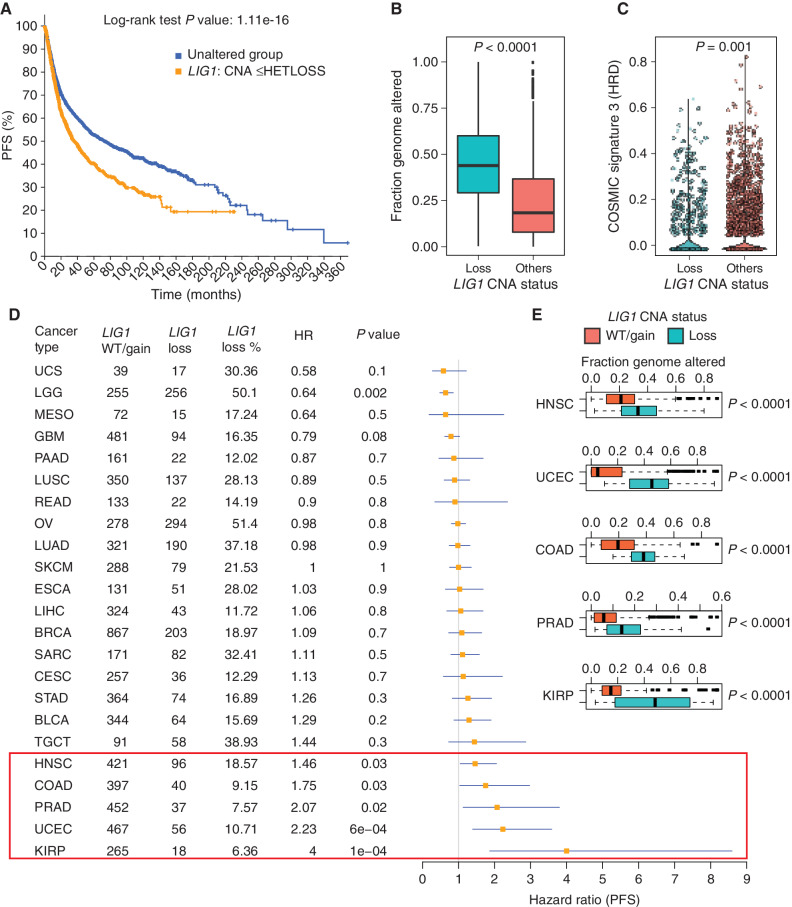
Microscaled proteogenomics was deployed to probe the molecular basis for differential response to neoadjuvant carboplatin and docetaxel combination chemotherapy for triple-negative breast cancer (TNBC). Proteomic analyses of pretreatment patient biopsies uniquely revealed metabolic pathways, including oxidative phosphorylation, adipogenesis, and fatty acid metabolism, that were associated with resistance. Both proteomics and transcriptomics revealed that sensitivity was marked by elevation of DNA repair, E2F targets, G2-M checkpoint, interferon-gamma signaling, and immune-checkpoint components. Proteogenomic analyses of somatic copy-number aberrations identified a resistance-associated 19q13.31-33 deletion where LIG1, POLD1, and XRCC1 are located. In orthogonal datasets, LIG1 (DNA ligase I) gene deletion and/or low mRNA expression levels were associated with lack of pathologic complete response, higher chromosomal instability index (CIN), and poor prognosis in TNBC, as well as carboplatin-selective resistance in TNBC preclinical models. Hemizygous loss of LIG1 was also associated with higher CIN and poor prognosis in other cancer types, demonstrating broader clinical implications.
Significance: Proteogenomic analysis of triple-negative breast tumors revealed a complex landscape of chemotherapy response associations, including a 19q13.31-33 somatic deletion encoding genes serving lagging-strand DNA synthesis (LIG1, POLD1, and XRCC1), that correlate with lack of pathologic response, carboplatin-selective resistance, and, in pan-cancer studies, poor prognosis and CIN. This article is highlighted in the In This Issue feature, p. 2483.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
![Figure 1. TNBC patient sample overview. A, REMARK diagram showing pre- and on-treatment sample accrual schema from patients with TNBC enrolled in two clinical trials [NCT02544987 (BCM) and NCT201404107 (WashU)] and treated with carboplatin and docetaxel in the neoadjuvant setting. *, <45% samples were later excluded from the analysis based on evidence from data quality control. B, Overview of available omics datasets from 59 patients (22 tumors with pCR and 37 tumors without pCR). Pathogenic BRCA1/2 and PALB2 mutation status, RCB, and patient race are indicated via color-coded annotation tracks. C, Venn diagram showing the overlap of gene IDs detected across multiple analytes and omics data profiled. SCNA, somatic copy-number alteration. D, Hallmark metabolism pathways are induced by chemotherapy exclusively at the protein level. Scatter plot shows signed −log10 FDR from GSEA using the signed (by direction of change) −log10 P values from paired Wilcoxon signed rank tests comparing RNA (x-axis) and protein levels (y-axis) for on-treatment (cycle 1, day 3) samples to matching baseline samples (n = 14).E, MSigDB Hallmark metabolism pathways are elevated in baseline non-pCR tumors at the protein level, whereas immune and cell-cycle pathways are elevated in baseline pCR tumors at both RNA and protein levels. Scatter plot shows the signed −log10 FDR values from GSEA using ranked lists of signed (by direction of change) −log10 P values from Wilcoxon rank sum tests comparing RNA (x-axis) and protein (y-axis) levels in non-pCR tumors to pCR tumors. F, Cell-cycle kinase targets and PTM-SigDB phosphosites associated with genotoxic stress are enriched in pCR tumors relative to non-pCR tumors at baseline. Volcano plot shows results from PTM-SEA using the signed −log10 P values from Wilcoxon rank sum tests comparing phosphosite levels in non-pCR tumors to pCR tumors. Red and blue dots indicate significant (FDR <0.05) posttranslational modification signatures.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/b639/9627136/be7e0eb15889/2586fig1.jpg)
![Figure 4. Discovery of DNA repair and replication components enriched in non-pCR TNBC tumors. A, Cytobands enriched in genes differentially expressed between non-pCR and pCR for both mRNA and protein. To identify upregulated or downregulated features overrepresented in certain cytobands within the chromosome, GSEA was used to identify regions from chromosomal location databases enriched with differential genes [GSEA input was ranked expression list (signed −log10 P value) from Wilcoxon rank sum tests]. Overrepresented cytobands that were either enriched or depleted using differentially expressed mRNA and protein are indicated in B, and the overlapping sets were used for further analysis. B, Plot showing significantly enriched or depleted cytobands obtained by running differential mRNA and protein ranked lists through GSEA. NES, normalized enrichment score. Genes downregulated in non-pCR samples corresponding to cytoband 19q13.31–33 are indicated in C. C, Venn diagram showing differential (non-pCR vs. pCR) mRNA and proteins located on cytoband 19q13.3. D, Overrepresentation analysis (ORA) shows that differential 19q13.31–33 genes are enriched with Hallmark DNA repair pathway genes. Downregulation of these DNA repair genes at the mRNA and protein levels in non-pCR cases is shown in the bar chart on the right as signed −log10 P values from Wilcoxon rank sum tests. E, Box plot comparing RNA expression of DNA repair genes located on 19q13.31–33 in the previously published BrighTNess clinical trial (treatment arms A and B), in which patients were treated with carboplatin and paclitaxel. The Wilcoxon rank sum test was used to compare residual disease (RD) cases with pCR cases. F, Forest plot showing hazard ratios (HR) and P values for metastasis-free survival associated with LIG1, POLD1, XRCC1, and ERCC2. HR is based on categorizing samples using a median expression cutoff for each gene in the Hatzis dataset.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/b639/9627136/dbbaa4db998e/2586fig4.jpg)
Comment in
References
-
- Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res 2007;13:4429–34. - PubMed
-
- Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med 2017;376:2147–59. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U54 CA224076/CA/NCI NIH HHS/United States
- R03 OD032626/OD/NIH HHS/United States
- U24 CA271075/CA/NCI NIH HHS/United States
- U24 CA270823/CA/NCI NIH HHS/United States
- P30 CA125123/CA/NCI NIH HHS/United States
- S10 OD028671/OD/NIH HHS/United States
- U24 CA210979/CA/NCI NIH HHS/United States
- U01 CA214125/CA/NCI NIH HHS/United States
- T32 CA203690/CA/NCI NIH HHS/United States
- P50 CA186784/CA/NCI NIH HHS/United States
- U24 CA210954/CA/NCI NIH HHS/United States
- U24 CA160034/CA/NCI NIH HHS/United States
- U24 CA210986/CA/NCI NIH HHS/United States
- K12 CA167540/CA/NCI NIH HHS/United States
- U24 CA226110/CA/NCI NIH HHS/United States
- U54 CA224083/CA/NCI NIH HHS/United States
- K22 CA241113/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
