

What is the Elbow Flexion Strength After Free Functional Gracilis Muscle Transfer for Adult Traumatic Complete Brachial Plexus Injuries?
- PMID: 36001032
- PMCID: PMC9653183
- DOI: 10.1097/CORR.0000000000002311
What is the Elbow Flexion Strength After Free Functional Gracilis Muscle Transfer for Adult Traumatic Complete Brachial Plexus Injuries?
Abstract
Background: Traumatic brachial plexus injuries (BPIs) in the nerve roots of C5 to T1 lead to the devastating loss of motor and sensory function in the upper extremity. Free functional gracilis muscle transfer (FFMT) is used to reconstruct elbow and shoulder function in adults with traumatic complete BPIs. The question is whether the gains in ROM and functionality for the patient outweigh the risks of such a large intervention to justify this surgery in these patients.
Questions/purposes: (1) After FFMT for adult traumatic complete BPI, what is the functional recovery in terms of elbow flexion, shoulder abduction, and wrist extension (ROM and muscle grade)? (2) Does the choice of distal insertion affect the functional recovery of the elbow, shoulder, and wrist? (3) Does the choice of nerve source affect elbow flexion and shoulder abduction recovery? (4) What factors are associated with less residual disability? (5) What proportion of flaps have necrosis and do not reinnervate?
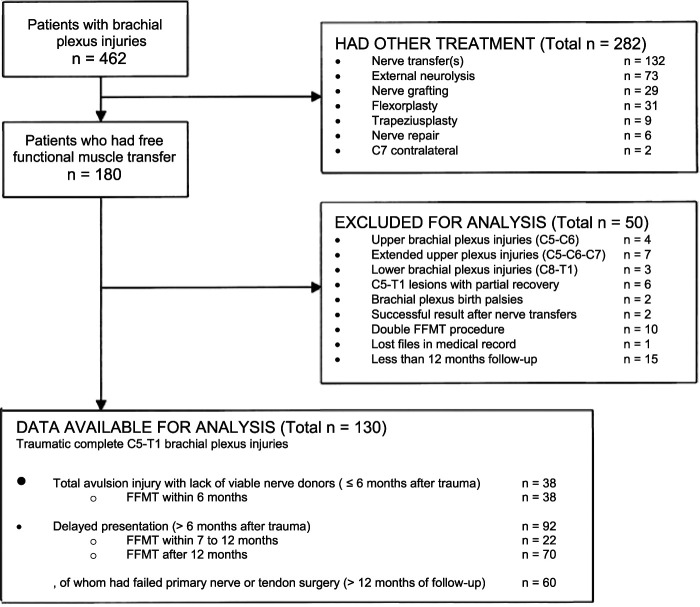
Methods: We performed a retrospective observational study at Dr. Soetomo General Hospital in Surabaya, Indonesia. A total of 180 patients with traumatic BPIs were treated with FFMT between 2010 and 2020, performed by a senior orthopaedic hand surgeon with 14 years of experience in FFMT. We included patients with traumatic complete C5 to T1 BPIs who underwent a gracilis FFMT procedure. Indications were total avulsion injuries and delayed presentation (>6 months after trauma) or after failed primary nerve transfers (>12 months). Patients with less than 12 months of follow-up were excluded, leaving 130 patients eligible for this study. The median postoperative follow-up period was 47 months (interquartile range [IQR] 33 to 66 months). Most were men (86%; 112 of 130) who had motorcycle collisions (96%; 125 patients) and a median age of 23 years (IQR 19 to 34 years). Orthopaedic surgeons and residents measured joint function at the elbow (flexion), shoulder (abduction), and wrist (extension) in terms of British Medical Research Council (MRC) muscle strength scores and active ROM. A univariate analysis of variance test was used to evaluate these outcomes in terms of differences in distal attachment to the extensor carpi radialis brevis (ECRB), extensor digitorum communis and extensor pollicis longus (EDC/EPL), the flexor digitorum profundus and flexor pollicis longus (FDP/FPL), and the choice of a phrenic, accessory, or intercostal nerve source. We measured postoperative function with the DASH score and pain at rest with the VAS score. A multivariate linear regression analysis was performed to investigate what patient and injury factors were associated with less disability. Complications such as flap necrosis, innervation problems, infections, and reoperations were evaluated.
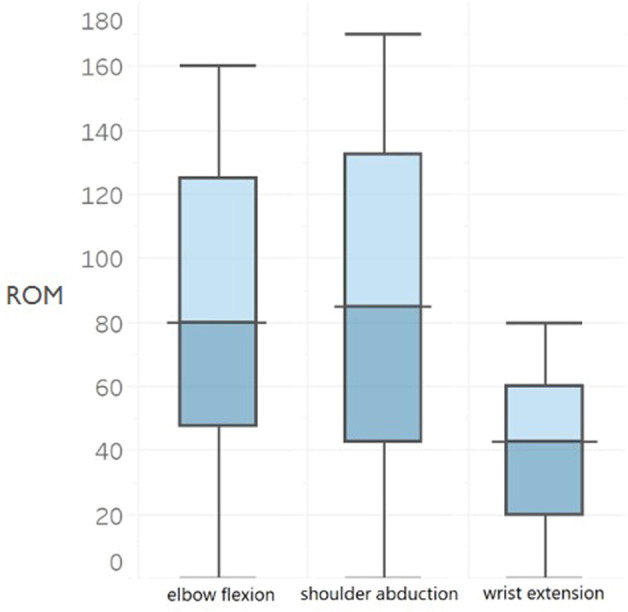
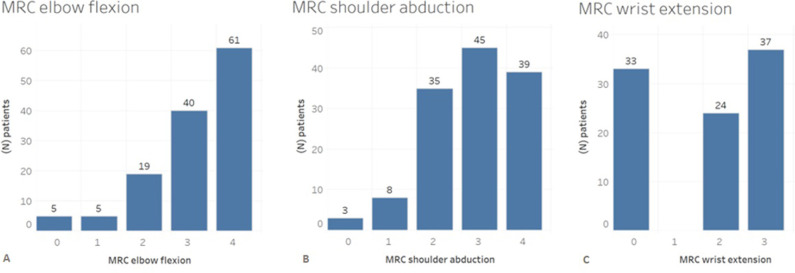
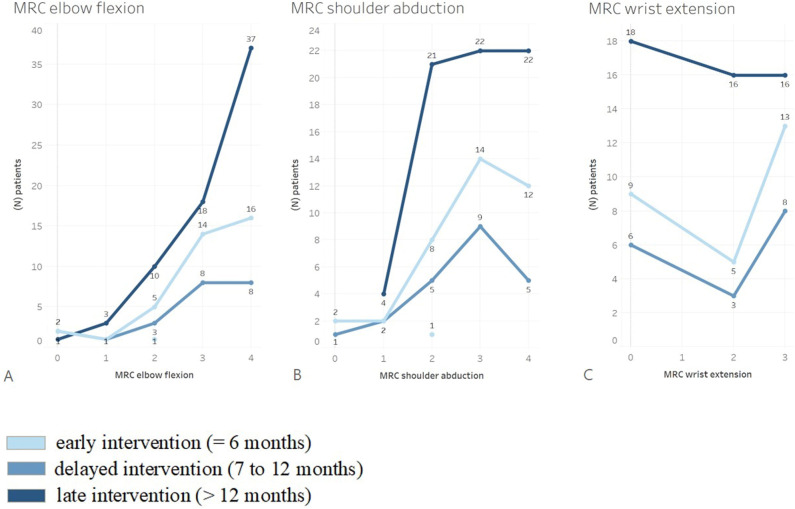
Results: The median elbow flexion muscle strength was 3 (IQR 3 to 4) and active ROM was 88° ± 46°. The median shoulder abduction grade was 3 (IQR 2 to 4) and active ROM was 62° ± 42°. However, the choice of distal insertion was not associated with differences in the median wrist extension strength (ECRB: 2 [IQR 0 to 3], EDC/EPL: 2 [IQR 0 to 3], FDP/FPL: 1 [IQR 0 to 2]; p = 0.44) or in ROM (ECRB: 21° ± 19°, EDC/EPL: 21° ± 14°, FDP/FPL: 13° ± 15°; p = 0.69). Furthermore, the choice of nerve source did not affect the mean ROM for elbow flexion (phrenic nerve: 87° ± 46°; accessory nerve: 106° ± 49°; intercostal nerves: 103° ± 50°; p = 0.55). No associations were found with less disability (lower DASH scores): young age (coefficient = 0.28; 95% CI -0.22 to 0.79; p = 0.27), being a woman (coefficient = -9.4; 95% CI -24 to 5.3; p = 0.20), and more postoperative months (coefficient = 0.02; 95% CI -0.01 to 0.05]; p = 0.13). The mean postoperative VAS score for pain at rest was 3 ± 2. Flap necrosis occurred in 5% (seven of 130) of all patients, and failed innervation of the gracilis muscle occurred in 4% (five patients).
Conclusion: FFMT achieves ROM with fair-to-good muscle power of elbow flexion, shoulder abduction, and overall function for the patient, but does not achieve good wrist function. Meticulous microsurgical skills and extensive rehabilitation training are needed to maximize the result of FFMT. Further technical developments in distal attachment and additional nerve procedures will pave the way for reconstructing a functional limb in patients with a flail upper extremity.
Level of evidence: Level III, therapeutic study.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures

Comment in
-
CORR Insights®: What is the Elbow Flexion Strength After Free Functional Gracilis Muscle Transfer for Adult Traumatic Complete Brachial Plexus Injuries?Clin Orthop Relat Res. 2022 Dec 1;480(12):2406-2408. doi: 10.1097/CORR.0000000000002407. Epub 2022 Sep 13. Clin Orthop Relat Res. 2022. PMID: 36099410 Free PMC article. No abstract available.
Similar articles
-
Free Functioning Gracilis Muscle Transfer With and Without Simultaneous Intercostal Nerve Transfer to Musculocutaneous Nerve for Restoration of Elbow Flexion After Traumatic Adult Brachial Pan-Plexus Injury.J Hand Surg Am. 2017 Apr;42(4):293.e1-293.e7. doi: 10.1016/j.jhsa.2017.01.014. Epub 2017 Feb 27. J Hand Surg Am. 2017. PMID: 28249790
-
Donor nerve sources in free functional gracilis muscle transfer for elbow flexion in adult brachial plexus injury.Microsurgery. 2017 Jul;37(5):377-382. doi: 10.1002/micr.30120. Epub 2016 Oct 5. Microsurgery. 2017. PMID: 27704606
-
Free Functioning Gracilis Muscle Transfer versus Intercostal Nerve Transfer to Musculocutaneous Nerve for Restoration of Elbow Flexion after Traumatic Adult Brachial Pan-Plexus Injury.Plast Reconstr Surg. 2016 Sep;138(3):483e-488e. doi: 10.1097/PRS.0000000000002471. Plast Reconstr Surg. 2016. PMID: 27556623
-
Gracilis free muscle transfer for restoration of function after complete brachial plexus avulsion.Neurosurg Focus. 2004 May 15;16(5):E8. doi: 10.3171/foc.2004.16.5.9. Neurosurg Focus. 2004. PMID: 15174828 Review.
-
Outcomes of gracilis free-flap muscle transfers and non-free-flap procedures for restoration of elbow flexion: A systematic review.J Plast Reconstr Aesthet Surg. 2022 Aug;75(8):2625-2636. doi: 10.1016/j.bjps.2022.04.025. Epub 2022 Apr 25. J Plast Reconstr Aesthet Surg. 2022. PMID: 35644885
Cited by
-
CORR Insights®: What is the Elbow Flexion Strength After Free Functional Gracilis Muscle Transfer for Adult Traumatic Complete Brachial Plexus Injuries?Clin Orthop Relat Res. 2022 Dec 1;480(12):2406-2408. doi: 10.1097/CORR.0000000000002407. Epub 2022 Sep 13. Clin Orthop Relat Res. 2022. PMID: 36099410 Free PMC article. No abstract available.
References
-
- Ahmed-Labib M, Golan JD, Jacques L. Functional outcome of brachial plexus reconstruction after trauma. Neurosurgery. 2007;61:1016-1022. - PubMed
-
- Akasara Y, Hara T, Takahashi M. Restoration of elbow flexion and wrist extension in brachial plexus paralyses by means of free muscle transplantation innervated by intercostal nerve. Ann Chir Main Memb Super. 1990;9:341-350. - PubMed
-
- Barrie K, Steinmann S, Shin A, Spinner R, Bishop A. Gracilis free muscle transfer for restoration of function after complete brachial plexus avulsion. Neurosurg Focus. 2004;16:E8. - PubMed
-
- Chalidapong P, Sananpanich K, Kraisarin J, Blumroongkit C. Pulmonary and biceps function after intercostal and phrenic nerve transfer for brachial plexus injuries. J Hand Surg Br. 2004;29:8-11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
