

Early Mortality in Type A Acute Aortic Dissection: Insights From the International Registry of Acute Aortic Dissection
- PMID: 36001309
- PMCID: PMC9403853
- DOI: 10.1001/jamacardio.2022.2718
Early Mortality in Type A Acute Aortic Dissection: Insights From the International Registry of Acute Aortic Dissection
Abstract
Importance: Early data revealed a mortality rate of 1% to 2% per hour for type A acute aortic dissection (TAAAD) during the initial 48 hours. Despite advances in diagnostic testing and treatment, this mortality rate continues to be cited because of a lack of contemporary data characterizing early mortality and the effect of timely surgery.
Objective: To examine early mortality rates for patients with TAAAD in the contemporary era.
Design, setting, and participants: This cohort study examined data for patients with TAAAD in the International Registry of Acute Aortic Dissection between 1996 and 2018. Patients were grouped according to the mode of their intended treatment, surgical or medical.
Exposure: Surgical treatment.
Main outcomes and measures: Mortality was assessed in the initial 48 hours after hospital arrival using Kaplan-Meier curves. In-hospital complications were also evaluated.
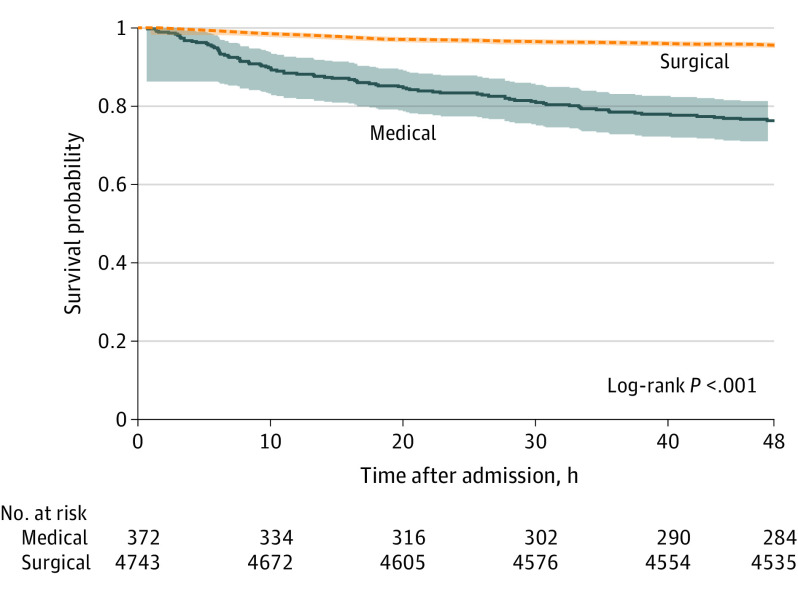
Results: A total of 5611 patients with TAAAD were identified based on intended treatment: 5131 (91.4%) in the surgical group (3442 [67.1%] male; mean [SD] age, 60.4 [14.1] years) and 480 (8.6%) in the medical group (480 [52.5%] male; mean [SD] age, 70.9 [14.7] years). Reasons for medical management included advanced age (n = 141), comorbidities (n = 281), and patient preference (n = 81). Over the first 48 hours, the mortality for all patients in the study was 5.8%. Among patients who were medically managed, mortality was 0.5% per hour (23.7% at 48 hours). For those whose intended treatment was surgical, 48-hour mortality was 4.4%. In the surgical group, 51 patients (1%) died before the operation.
Conclusions and relevance: In this study, the overall mortality rate for TAAAD was 5.8% at 48 hours. For patients in the medical group, TAAAD had a mortality rate of 0.5% per hour (23.7% at 48 hours). However, among those in the surgical group, 48-hour mortality decreased to 4.4%.
Conflict of interest statement
Figures
References
-
- Hiratzka LF, Bakris GL, Beckman JA, et al. ; American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines; American Association for Thoracic Surgery; American College of Radiology; American Stroke Association; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society of Thoracic Surgeons; Society for Vascular Medicine . 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease. J Am Coll Cardiol. 2010;55(14):e27-e129. doi:10.1016/j.jacc.2010.02.015 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
