

Decongestion Models and Metrics in Acute Heart Failure: ESCAPE Data in the Age of the Implantable Cardiac Pressure Monitor
- PMID: 36001949
- PMCID: PMC9427063
- DOI: 10.14503/THIJ-21-7587
Decongestion Models and Metrics in Acute Heart Failure: ESCAPE Data in the Age of the Implantable Cardiac Pressure Monitor
Abstract
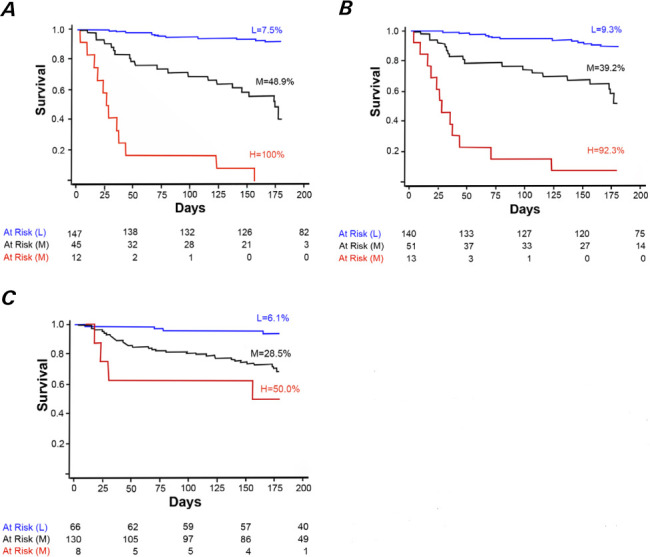
The United States Food and Drug Administration restricts the use of implantable cardiac pressure monitors to patients with New York Heart Association (NYHA) class III heart failure (HF). We investigated whether single-pressure monitoring could predict survival in HF patients as part of a model constructed using data from the ESCAPE (Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness) trial. We validated survival models in 204 patients, using all-cause 180-day mortality. Two levels of model complexity were tested: 1) a simplified 1-pressure model based on pulmonary artery mean pressure ([PAM]1P) (information obtainable from an implanted intracardiac monitor alone), and 2) a pair of 5-variable risk score models based on right atrial pressure (RAP) + pulmonary capillary wedge pressure (PCWP) ([RAP+PCWP]5V) and on RAP + PAM ([RAP+PAM]5V). The more complex models used 5 dichotomous variables: a congestion index above a certain threshold value, baseline systolic blood pressure of <100 mmHg, baseline blood urea nitrogen level of ≥ 34 mg/dL, need for cardiopulmonary resuscitation or mechanical ventilation, and posttreatment NYHA class IV status. The congestion index was defined as posttreatment RAP+PCWP or posttreatment RAP+PAM, with congestion thresholds of 34 and 42 mmHg, respectively (median pulmonary catheter indwelling time, 1.9 d). The 5-variable models predicted survival with areas under the curve of 0.868 for the (RAP+PCWP)5V model and 0.827 for the (RAP+PAM)5V model, whereas the 1-pressure model predicted survival with an area under the curve of 0.718. We conclude that decongestion as determined by hemodynamic assessment predicts survival in HF patients and that it may be the final pathway for treatment benefit despite improvements in pharmacologic intervention since the ESCAPE trial.
Keywords: Acute heart failure/diagnosis/mortality/therapy; blood pressure monitors; cardiovascular models; hemodynamics; monitoring, physiologic/instrumentation; risk assessment; survival.
© 2022 by the Texas Heart® Institute, Houston.
Conflict of interest statement
Figures
Similar articles
-
Usefulness of the Sum of Pulmonary Capillary Wedge Pressure and Right Atrial Pressure as a Congestion Index that Prognosticates Heart Failure Survival (from the Evaluation Study of Congestive Heart Failure and Pulmonary Artery Catheterization Effectiveness Trial).Am J Cardiol. 2016 Sep 15;118(6):854-859. doi: 10.1016/j.amjcard.2016.06.040. Epub 2016 Jun 28. Am J Cardiol. 2016. PMID: 27474338
-
Relationship of right- to left-sided ventricular filling pressures in advanced heart failure: insights from the ESCAPE trial.Circ Heart Fail. 2013 Mar;6(2):264-70. doi: 10.1161/CIRCHEARTFAILURE.112.000204. Epub 2013 Feb 7. Circ Heart Fail. 2013. PMID: 23392790
-
Congestion patterns in severe tricuspid regurgitation and transcatheter treatment: Insights from a multicentre registry.Eur J Heart Fail. 2024 Apr;26(4):1004-1014. doi: 10.1002/ejhf.3235. Epub 2024 Apr 4. Eur J Heart Fail. 2024. PMID: 38571456
-
Advanced Markers for Hemodynamic Monitoring in Cardiogenic Shock and End-Stage Heart Failure: A Mini Review.Heart Fail Rev. 2025 May;30(3):529-535. doi: 10.1007/s10741-025-10483-5. Epub 2025 Jan 14. Heart Fail Rev. 2025. PMID: 39808367 Review.
-
Early and medium term results of tailored therapy for heart failure.Rev Port Cardiol. 2001 Mar;20(3):261-82. Rev Port Cardiol. 2001. PMID: 11417309 Review. English, Portuguese.
References
-
- Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol . 2022;79(17):e263–e421. - PubMed
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail . 2016;18(8):891–975. - PubMed
-
- Abraham WT, Stevenson LW, Bourge RC, Lindenfeld JA, Bauman JG, Adamson PB, CHAMPION Trial Study Group Sustained efficacy of pulmonary artery pressure to guide adjustment of chronic heart failure therapy: complete follow-up results from the CHAMPION randomised trial. Lancet . 2016;387(10017):453–61. - PubMed
-
- Hindricks G, Taborsky M, Glikson M, Heinrich U, Schumacher B, Katz A et al. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet . 2014;384(9943):583–90. - PubMed
-
- Binanay C, Califf RM, Hasselblad V, O'Connor CM, Shah MR, Sopko G et al. Evaluation study of congestive heart failure and pulmonary artery catheterization effectiveness: the ESCAPE trial. JAMA . 2005;294(13):1625–33. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
