

2022 AAFP/EveryCat Feline Infectious Peritonitis Diagnosis Guidelines
- PMID: 36002137
- PMCID: PMC10812230
- DOI: 10.1177/1098612X221118761
2022 AAFP/EveryCat Feline Infectious Peritonitis Diagnosis Guidelines
Erratum in
-
Erratum to '2022 AAFP/EveryCat Feline Infectious Peritonitis Diagnosis Guidelines'.J Feline Med Surg. 2022 Dec;24(12):e676. doi: 10.1177/1098612X221126448. Epub 2022 Sep 6. J Feline Med Surg. 2022. PMID: 36066350 Free PMC article. No abstract available.
Abstract
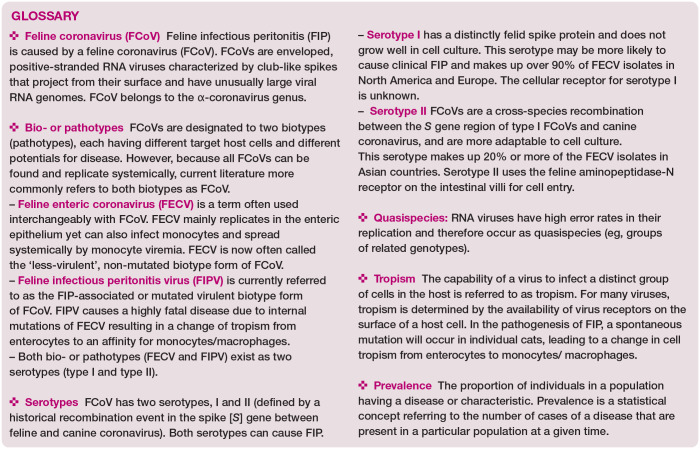
Clinical importance: Feline infectious peritonitis (FIP) is one of the most important infectious diseases and causes of death in cats; young cats less than 2 years of age are especially vulnerable. FIP is caused by a feline coronavirus (FCoV). It has been estimated that around 0.3% to 1.4% of feline deaths at veterinary institutions are caused by FIP.
Scope: This document has been developed by a Task Force of experts in feline clinical medicine as the 2022 AAFP/EveryCat Feline Infectious Peritonitis Diagnosis Guidelines to provide veterinarians with essential information to aid their ability to recognize cats presenting with FIP.
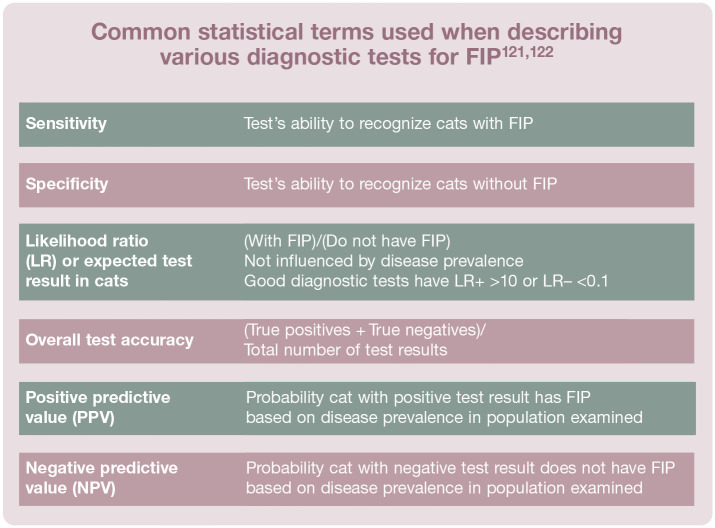
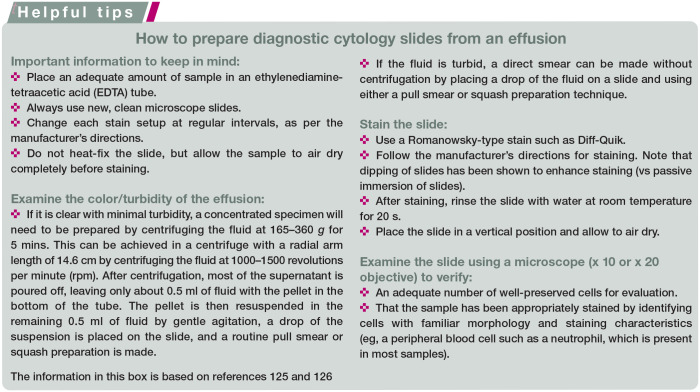
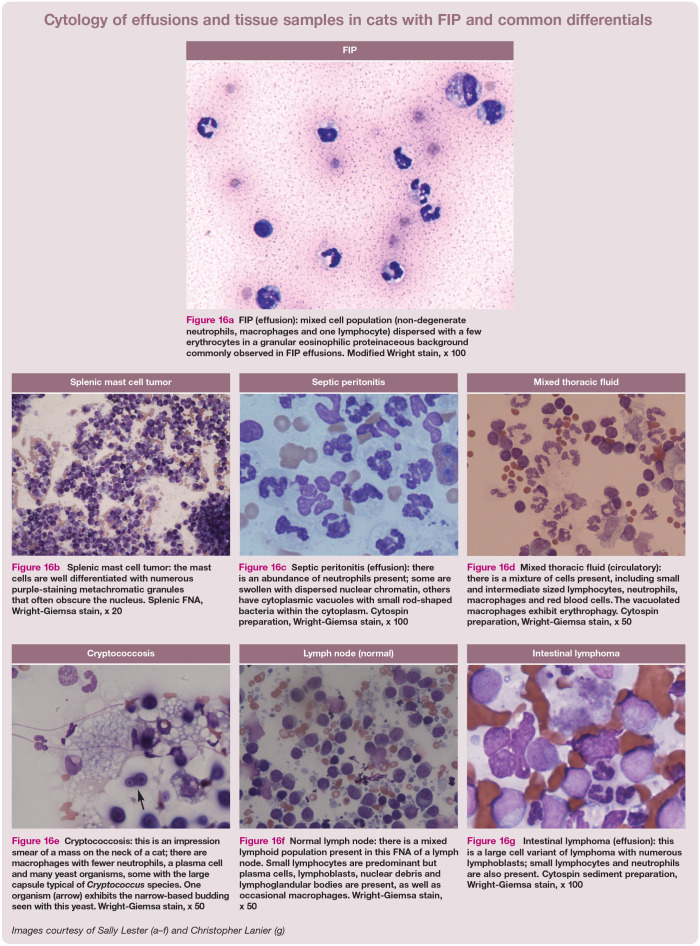
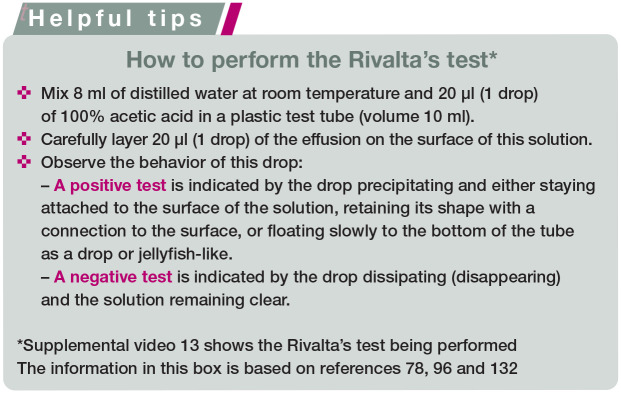
Testing and interpretation: Nearly every small animal veterinary practitioner will see cases. FIP can be challenging to diagnose owing to the lack of pathognomonic clinical signs or laboratory changes, especially when no effusion is present. A good understanding of each diagnostic test's sensitivity, specificity, predictive value, likelihood ratio and diagnostic accuracy is important when building a case for FIP. Before proceeding with any diagnostic test or commercial laboratory profile, the clinician should be able to answer the questions of 'why this test?' and 'what do the results mean?' Ultimately, the approach to diagnosing FIP must be tailored to the specific presentation of the individual cat.
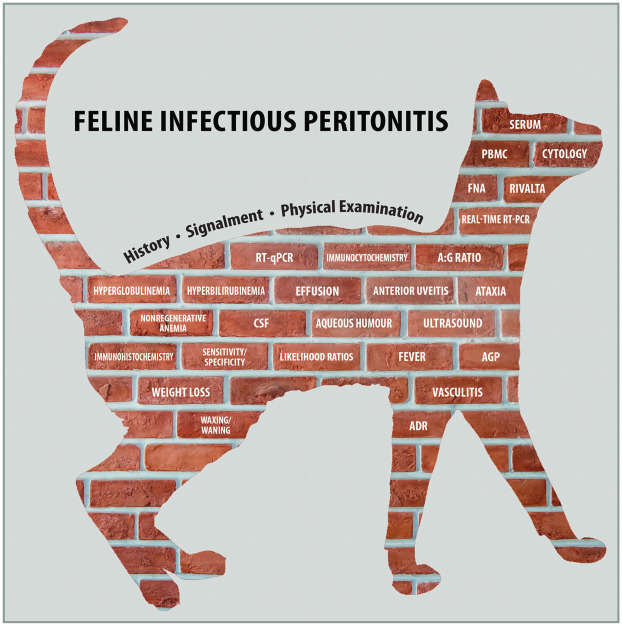
Relevance: Given that the disease is fatal when untreated, the ability to obtain a correct diagnosis is critical. The clinician must consider the individual patient's history, signalment and comprehensive physical examination findings when selecting diagnostic tests and sample types in order to build the index of suspicion 'brick by brick'. Research has demonstrated efficacy of new antivirals in FIP treatment, but these products are not legally available in many countries at this time. The Task Force encourages veterinarians to review the literature and stay informed on clinical trials and new drug approvals.
Keywords: AFAST; FCoV; FIP; Feline infectious peritonitis; PCR; PCR testing; RNA; RNA virus; Rivalta; analysis; antibody; blood test; cytology; diagnosis; effusion; feline coronavirus; fluid; imaging; infection; laboratory sample; lesion; polymerase chain reaction; screening; virus.
Conflict of interest statement
The Task Force members have no conflicts of interest to declare.
Figures











References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
