

Local variation in low carbon footprint inhalers in pre-COVID pandemic primary care prescribing guidelines for adult asthma in England and its potential impact
- PMID: 36002398
- PMCID: PMC9825955
- DOI: 10.1111/bcp.15511
Local variation in low carbon footprint inhalers in pre-COVID pandemic primary care prescribing guidelines for adult asthma in England and its potential impact
Abstract
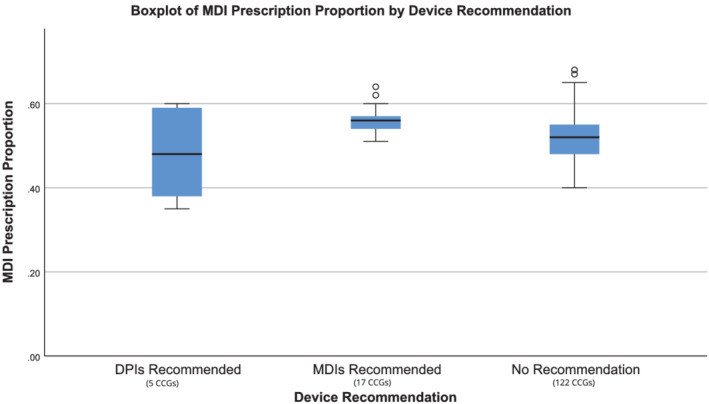
Aims: Pressurised metered-dose inhalers (MDIs) have a much higher carbon footprint than dry powder inhalers (DPIs). We aimed to describe variations of inhaler options in local adult asthma prescribing guidance.
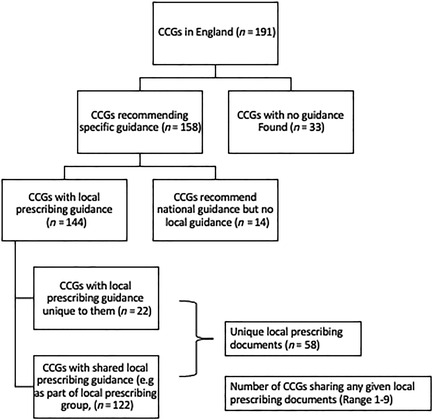
Methods: We reviewed local clinical commissioning group (CCG) adult asthma prescribing guidance for primary care in England in 2019 and recorded DPI and MDI inclusion. The relationship to prescribing data from OpenPrescribing.net was examined.
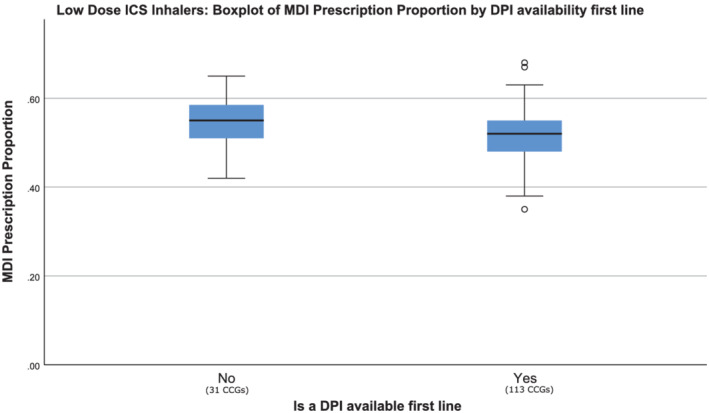
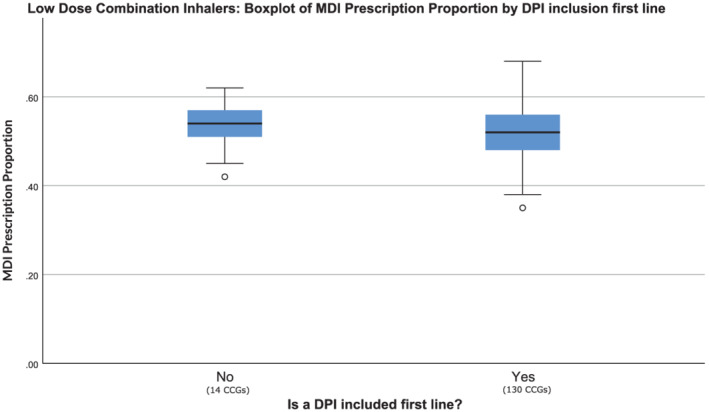
Results: In total, 58 unique guidance documents were analysed covering 144 out of 191 CCGs in England. Only 3% of CCG guidelines expressed an overall preference for DPIs, while 12% explicitly preferred MDIs. The inclusion of DPIs first-line was 77% for short-acting β-agonists, 78% for low-dose inhaled corticosteroid (ICS) inhalers and 90-96% for combination long-acting β-agonist/ICS inhalers. MDIs were included first-line in 98-100% of these classes. In 26% of CCGs, there was no first-line DPI option for at least 1 asthma management step. Ten percent of CCGs had no DPI included first-line for any of the 5 classes examined. Many CCGs recommended higher carbon footprint options; Ventolin MDI (25.6%), inhalers containing HFA227ea (57.9%) and ICS regimes recommending 2 puffs of a lower dose over 1 puff of higher dose (94.2%). MDIs were prescribed more in CCGs that recommended them.
Conclusion: Before the COVID pandemic, there was substantial variation between CCGs in adult asthma prescribing guidance regarding higher and lower carbon footprint options. There may still be scope to amend local guidance to improve clinical and environmental outcomes. This study provides a method and baseline for further investigation of this.
Keywords: asthma; climate change; prescribing; respiratory medicine.
© 2022 The Authors. British Journal of Clinical Pharmacology published by John Wiley & Sons Ltd on behalf of British Pharmacological Society.
Figures
References
-
- The NHS Net Zero Expert Panel. Delivering a ‘Net Zero’ National Health Service . NHS. Published online 2020:12. https://www.england.nhs.uk/greenernhs/wp-content/uploads/sites/51/2020/1...
-
- Fulford B, Mezzi K, Whiting A, Aumônier S. Life‐Cycle Assessment of the Breezhaler® Breath‐Actuated Dry Powder Inhaler. Sustainability. 2021;13(12):6657. doi:10.3390/SU13126657 - DOI
