

A case of early onset adenocarcinoma associated with colorectal polyposis with an unknown germline mutation
- PMID: 36002671
- PMCID: PMC9402821
- DOI: 10.1186/s40792-022-01518-2
A case of early onset adenocarcinoma associated with colorectal polyposis with an unknown germline mutation
Abstract
Background: Typically, in cases of adenomatous polyposis, colorectal cancer develops in the third or fourth decade of life. We report the case of a female patient with colorectal polyposis who developed adenocarcinoma at 8 years of age.
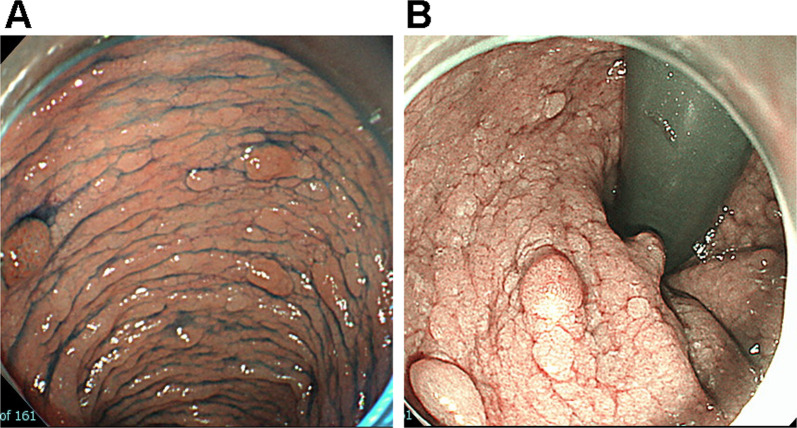
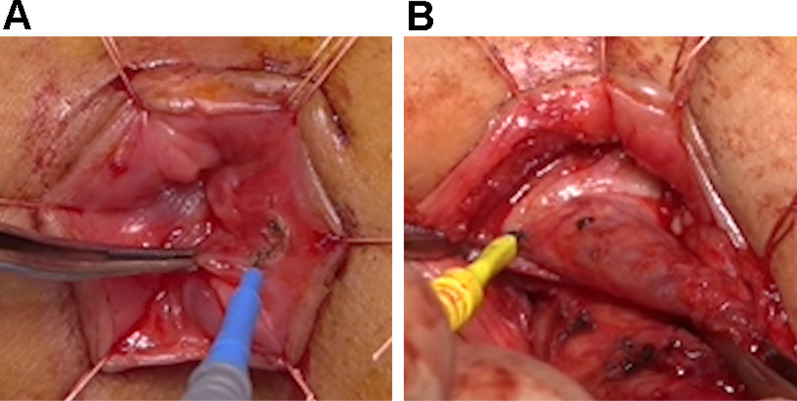
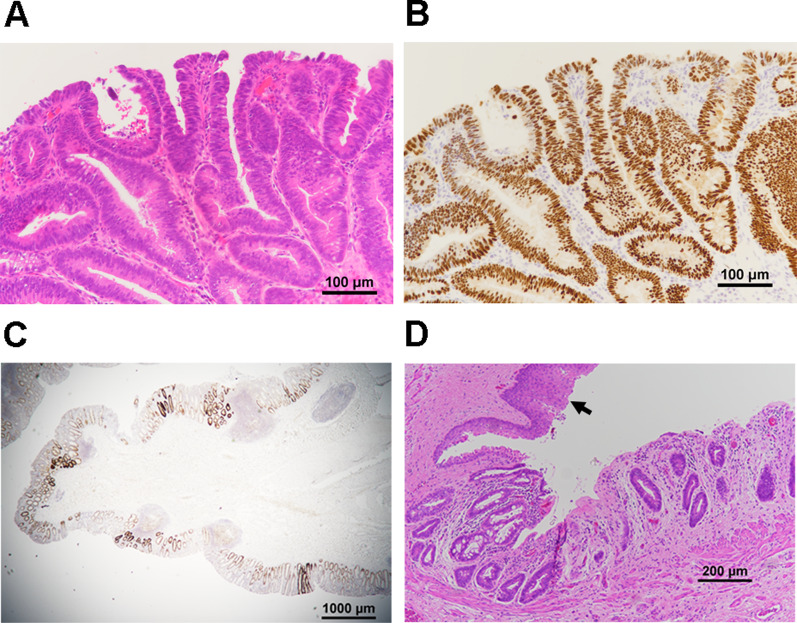
Case presentation: An 8-year-old girl was admitted with a 4-year history of occasional bloody stools. Colonoscopy revealed colon polyposis and histopathological assessment confirmed a well-differentiated adenocarcinoma in the adenomatous polyps, so laparoscopy-assisted proctocolectomy was performed in the lithotomy position by a simultaneous abdominal and anal approach. To completely resect the rectal mucosa, excision was commenced just distal to the dentate line. After the mucosal resection up to the peritoneal reflection level, an inverted muscular cuff was cut circumferentially, and the terminal ileum was pulled through the muscular cuff and anastomosed to the anal canal. Histopathology revealed multiple adenomatous polyps and scattered well-differentiated tubular adenocarcinomas (tub1) in the adenomatous polyps and the non-polypoid mucosal lesions. Because complete resection was achieved, additional adjuvant chemotherapy was not administered. Polymerase chain reaction (PCR)-direct sequencing of the entire coding region and the exon-intron junctions, and real-time PCR of DNA extracted from blood cells, revealed no mutations of either APC or MUTYH. No deletions, duplications, translocations or inversions of APC, MUTYH and GREM1 genes were found using multiplex ligation-dependent probe amplification (MLPA) and G-banding analysis. Multi-gene panels sequencing for polyposis syndromes or hereditary colorectal cancers, and trio-whole exome sequencing was conducted. However, no candidate pathogenic variants of genes were detected in de novo dominant or autosomal recessive model. Somatic mutation of APC was not detected in 4 polyps by loss of heterozygosity analysis at a single nucleotide polymorphism in intron 14. The patient has remained disease-free for 5 years. Currently, the patient is on loperamide and passes stool 5 times/day without any soiling.
Conclusions: The genetic analysis suggests that she may have a germline mutation at unscreened region of these genes or in unidentified FAP gene. The patient will be carefully followed up for residual rectal carcinoma and for the development of other cancers.
Keywords: Adenocarcinoma; Children; Mutation; Pediatric; Polyposis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
De novo familial adenomatous polyposis with germline double heterozygosity of APC/BRCA2: a case report and literature review.Hered Cancer Clin Pract. 2025 Feb 21;23(1):6. doi: 10.1186/s13053-025-00306-x. Hered Cancer Clin Pract. 2025. PMID: 39985003 Free PMC article.
-
Curative resection via right hemicolectomy and regional lymph node dissection for colonic adenomatous polyposis of unknown etiology with adenocarcinomas localized in the right side of the colon: a case report.Surg Case Rep. 2024 Apr 22;10(1):93. doi: 10.1186/s40792-024-01890-1. Surg Case Rep. 2024. PMID: 38647838 Free PMC article.
-
Contribution of APC and MUTYH mutations to familial adenomatous polyposis susceptibility in Hungary.Fam Cancer. 2016 Jan;15(1):85-97. doi: 10.1007/s10689-015-9845-5. Fam Cancer. 2016. PMID: 26446593 Free PMC article.
-
Familial adenomatous polyposis.Orphanet J Rare Dis. 2009 Oct 12;4:22. doi: 10.1186/1750-1172-4-22. Orphanet J Rare Dis. 2009. PMID: 19822006 Free PMC article. Review.
-
Juvenile polyposis syndrome might be misdiagnosed as familial adenomatous polyposis: a case report and literature review.BMC Gastroenterol. 2020 Jun 1;20(1):167. doi: 10.1186/s12876-020-01238-7. BMC Gastroenterol. 2020. PMID: 32487124 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
