

Long-term outcomes of laparoscopic Extralevator Abdominoperineal excision with modified position change for low rectal Cancer treatment
- PMID: 36002810
- PMCID: PMC9404665
- DOI: 10.1186/s12885-022-10019-2
Long-term outcomes of laparoscopic Extralevator Abdominoperineal excision with modified position change for low rectal Cancer treatment
Abstract
Background: Extralevator abdominoperineal excision (ELAPE) has been recommended for treating low rectal cancer due to its potential advantages in improving surgical safety and oncologic outcomes as compared to conventional abdominoperineal excision (APE). In ELAPE, however, whether the benefits of intraoperative position change to a prone jackknife position outweighs the associated risks remains controversial. This study is to introduce a modified position change in laparoscopic ELAPE and evaluate its feasibility, safety and the long-term therapeutic outcomes.
Methods: Medical records of 56 consecutive patients with low rectal cancer underwent laparoscopic ELAPE from November 2013 to September 2016 were retrospectively studied. In the operation, a perineal dissection in prone jackknife position was firstly performed and the laparoscopic procedure was then conducted in supine position. Patient characteristics, intraoperative and postoperative outcomes, pathologic and 5-year oncologic outcomes were analyzed.
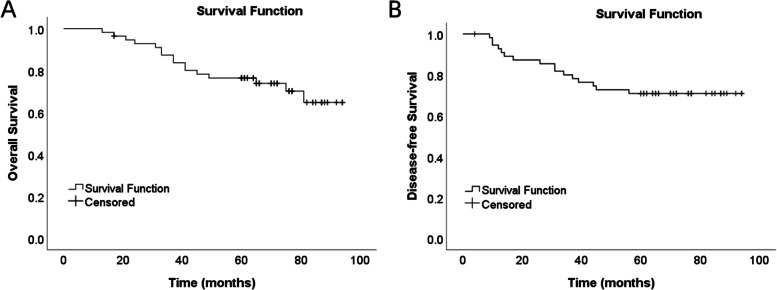
Results: The mean operation time was 213.5 ± 29.4 min and the mean intraoperative blood loss was 152.7 ± 125.2 ml. All the tumors were totally resected, without intraoperative perforation, conversion to open surgery, postoperative 30-day death, and perioperative complications. All the patients achieved pelvic peritoneum reconstruction without the usage of biological mesh. During the follow-up period, perineal hernia was observed in 1 patient, impaired sexual function in 1 patient, and parastomal hernias in 3 patients. The local recurrence rate was 1.9% and distant metastasis was noted in 12 patients. The 5-year overall survival rate was 76.4% and the 5-year disease-free survival rate was 70.9%.
Conclusions: Laparoscopic ELAPE with modified position change is a simplified, safe and feasible procedure with favorable outcomes. The pelvic peritoneum can be directly closed by the laparoscopic approach without the application of biological mesh.
Keywords: Exralevator abdominoperineal resection; Long-term; Low rectal cancer; Position change; Survival analysis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Extralevator abdominoperineal excision for advanced low rectal cancer: Where to go.World J Gastroenterol. 2020 Jun 14;26(22):3012-3023. doi: 10.3748/wjg.v26.i22.3012. World J Gastroenterol. 2020. PMID: 32587445 Free PMC article. Review.
-
[Feasibility and short-outcomes of laparoscopic extralevator abdominoperineal excision without changing position for distal rectal cancer].Zhonghua Wai Ke Za Zhi. 2014 Nov;52(11):826-30. Zhonghua Wai Ke Za Zhi. 2014. PMID: 25604020 Chinese.
-
Transabdominal extralevator abdominoperineal excision (eLAPE) performed by laparoscopic approach with no position change.J Laparoendosc Adv Surg Tech A. 2015 Mar;25(3):202-6. doi: 10.1089/lap.2014.0413. Epub 2015 Feb 6. J Laparoendosc Adv Surg Tech A. 2015. PMID: 25658808
-
Is it worthwhile to perform closure of the pelvic peritoneum in laparoscopic extralevator abdominoperineal resection?Langenbecks Arch Surg. 2022 May;407(3):1139-1150. doi: 10.1007/s00423-021-02412-5. Epub 2022 Jan 27. Langenbecks Arch Surg. 2022. PMID: 35083567
-
Controversies in abdominoperineal excision.Surg Oncol Clin N Am. 2014 Jan;23(1):93-111. doi: 10.1016/j.soc.2013.09.005. Surg Oncol Clin N Am. 2014. PMID: 24267168 Review.
References
-
- den Dulk M, Putter H, Collette L, Marijnen C, Folkesson J, Bosset JF, et al. The abdominoperineal resection itself is associated with an adverse outcome: the European experience based on a pooled analysis of five European randomised clinical trials on rectal cancer. Eur J Cancer. 2009;45(7):1175–1183. doi: 10.1016/j.ejca.2008.11.039. - DOI - PubMed
MeSH terms
Grants and funding
- 2015FZA01005/Weihai Municipal Science and Technology Foundation
- 2015FZA01005/Weihai Municipal Science and Technology Foundation
- 2015FZA01005/Weihai Municipal Science and Technology Foundation
- 2015FZA01005/Weihai Municipal Science and Technology Foundation
- 2015FZA01005/Weihai Municipal Science and Technology Foundation
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
