

Changes in analgesic strategies for lobectomy from 2009 to 2018
- PMID: 36003558
- PMCID: PMC9390760
- DOI: 10.1016/j.xjon.2021.03.015
Changes in analgesic strategies for lobectomy from 2009 to 2018
Abstract
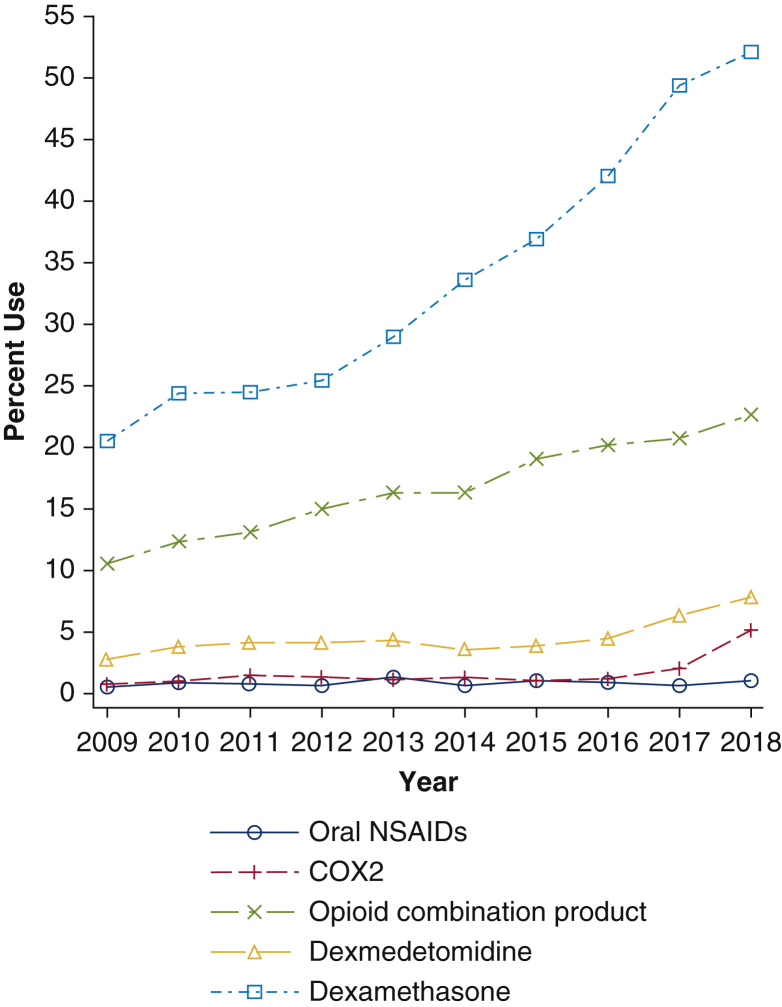
Objective: To evaluate trends in the use of epidural analgesia and nonopioid and opioid analgesics for patients undergoing lobectomy from 2009 to 2018.
Methods: We queried the Premier database for adult patients undergoing open, video-assisted, and robotic-assisted lobectomy from 2009 to 2018. The outcome of interest was changes in the receipt of epidural analgesia and nonopioid and opioid analgesics as measured by charges on the day of surgery. We also evaluated postoperative daily opioid use. We used multivariable logistic and linear regression models to examine the association between the utilization of each analgesic modality and year.
Results: We identified 86,308 patients undergoing lobectomy from 2009 to 2018 within the Premier database: 35,818 (41.5%) patients had open lobectomy, 35,951 (41.7%) patients had video-assisted lobectomy, and 14,539 (16.8%) patients had robotic-assisted lobectomy. For all 3 surgical cohorts, epidural analgesia use decreased, and nonopioid analgesics use increased over time, except for intravenous nonsteroidal anti-inflammatory drugs. Use of patient-controlled analgesia decreased, while opioid consumption on the day of surgery increased and postoperative opioid consumption did not decrease over time.
Conclusions: In this large sample of patients undergoing lobectomy, utilization of epidural analgesia declined and use of nonopioid analgesics increased. Despite these changes, opioid consumption on day of surgery increased, and there was no significant reduction in postoperative opioid consumption. Further research is warranted to examine the association of these changes with patient outcomes.
Keywords: COX-2, cyclooxygenase-2; FDA, Food and Drug Administration; ICD, International Classification of Diseases; IV, intravenous; NSAID, nonsteroidal anti-inflammatory drug; PCA, patient-controlled analgesia; PME, parental morphine equivalent; PO, per os, oral; POD, postoperative day; RATS, robotic-assisted thoracoscopic surgery; VATS, video-assisted thoracoscopic surgery; epidural analgesia; lobectomy; multimodal analgesia; nonopioid analgesia; robotic-assisted thoracoscopic surgery; thoracic surgery; thoracotomy; video-assisted thoracoscopic surgery.
© 2021 The Author(s).
Figures











Similar articles
-
Continuous erector spinae plane block versus thoracic epidural analgesia in video-assisted thoracic surgery: a study protocol for a prospective randomized open label non-inferiority trial.Trials. 2021 May 4;22(1):321. doi: 10.1186/s13063-021-05275-9. Trials. 2021. PMID: 33947442 Free PMC article.
-
Regional versus systemic analgesia in video-assisted thoracoscopic lobectomy: a retrospective analysis.BMC Anesthesiol. 2019 Oct 17;19(1):183. doi: 10.1186/s12871-019-0851-2. BMC Anesthesiol. 2019. PMID: 31623571 Free PMC article.
-
Is epidural analgesia necessary after video-assisted thoracoscopic lobectomy?Asian Cardiovasc Thorac Ann. 2010 Oct;18(5):464-8. doi: 10.1177/0218492310381817. Asian Cardiovasc Thorac Ann. 2010. PMID: 20947601
-
[Multimodal Analgesia of Enhanced Recovery after Surgery Management in Lobectomy by Video-assisted Thoracoscopic Surgery].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021 Feb 28;43(1):136-143. doi: 10.3881/j.issn.1000-503X.12758. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021. PMID: 33663675 Review. Chinese.
-
A systematic review and meta-analysis of robotic versus open and video-assisted thoracoscopic surgery approaches for lobectomy.Interact Cardiovasc Thorac Surg. 2019 Apr 1;28(4):526-534. doi: 10.1093/icvts/ivy315. Interact Cardiovasc Thorac Surg. 2019. PMID: 30496420
Cited by
-
Commentary: Waves of pain.JTCVS Open. 2021 Apr 20;6:239-240. doi: 10.1016/j.xjon.2021.04.001. eCollection 2021 Jun. JTCVS Open. 2021. PMID: 36003573 Free PMC article. No abstract available.
-
Commentary: Leaders float all boats higher and faster.JTCVS Open. 2021 Apr 30;6:237-238. doi: 10.1016/j.xjon.2021.04.012. eCollection 2021 Jun. JTCVS Open. 2021. PMID: 36003579 Free PMC article. No abstract available.
-
Deep learning models for the prediction of acute postoperative pain in PACU for video-assisted thoracoscopic surgery.BMC Med Res Methodol. 2024 Oct 7;24(1):232. doi: 10.1186/s12874-024-02357-5. BMC Med Res Methodol. 2024. PMID: 39375589 Free PMC article.
References
-
- Wenk M., Schug S.A. Perioperative pain management after thoracotomy. Curr Opin Anaesthesiol. 2011;24:8–12. - PubMed
-
- Richebe P., Capdevila X., Rivat C. Persistent postsurgical pain: pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129:590–607. - PubMed
-
- Kaiser A.M., Zollinger A., De Lorenzi D., Largiadèr F., Weder W. Prospective, randomized comparison of extrapleural versus epidural analgesia for postthoracotomy pain. Ann Thorac Surg. 1998;66:367–372. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
