

Impact of early surgical correction or palliation of congenital heart defects in infants with symptomatic viral respiratory tract infections in the current era
- PMID: 36003574
- PMCID: PMC9390683
- DOI: 10.1016/j.xjon.2021.03.009
Impact of early surgical correction or palliation of congenital heart defects in infants with symptomatic viral respiratory tract infections in the current era
Abstract
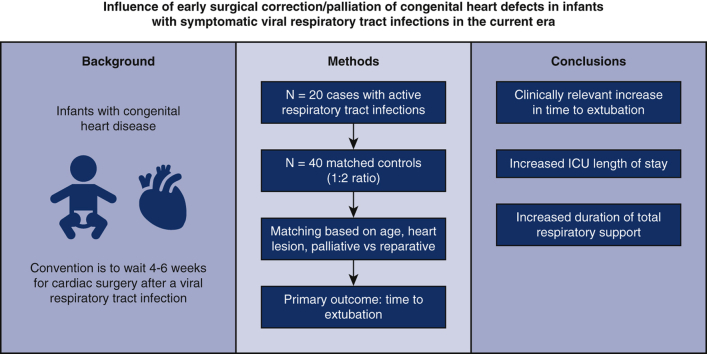
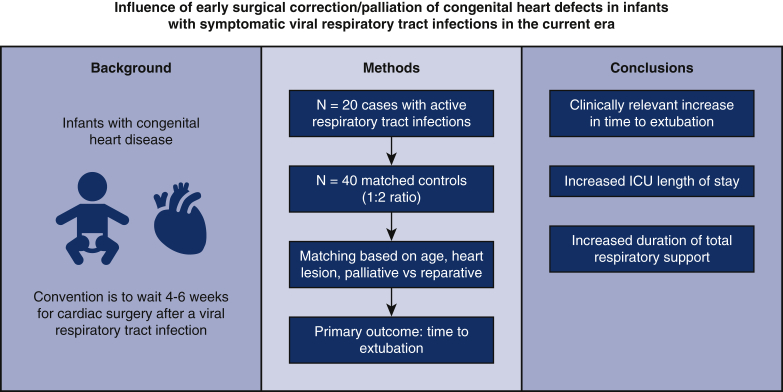
Objective: This study investigates the influence of timing of surgery among infants with congenital heart disease and active respiratory tract infections in a contemporary Western Canadian cohort.
Methods: This was a retrospective matched cohort study of infants aged 1 week to 6 months undergoing surgical repair of congenital heart disease between 2014 and 2017. Case patients had active respiratory tract infections preoperatively and were matched to control patients based on primary heart lesion. The primary outcome was time to extubation.
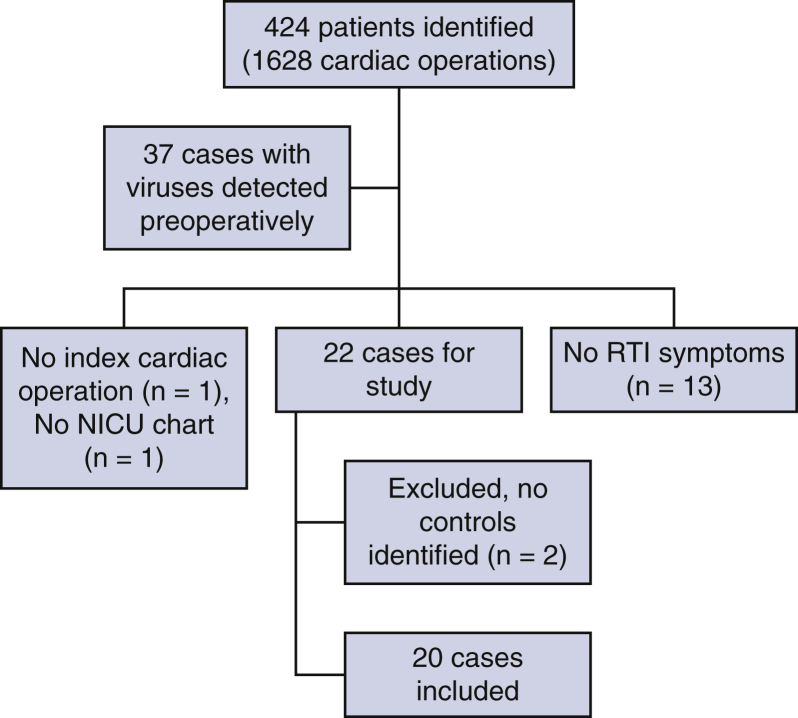
Results: We identified 20 cases (median age, 3.4 months [range, 2.4-4.3 months]) that were matched to 40 controls (1:2 ratio). In case patients, surgery occurred at a median of 1 day after the positive viral testing. There were no statistically significant differences between cases and controls in time to extubation (59 vs 34 hours [P = .12]), postoperative vasoactive scores at 24 hours (0 vs 0 [P = .53]), 48 hours (0 vs 0 [P = .23]), maximum vasoactive score in postoperative period (5 vs 5.5 [P = .54]), or time to hospital discharge (13 vs 12 days [P = .39]). Case patients had increased duration of total respiratory support (including noninvasive ventilation, 3.5 vs 2 days [P = .02]) and postoperative intensive care unit length of stay (5.5 vs 3 days [P = .01]).
Conclusions: Cardiac surgery on infants with congenital heart disease during an acute viral respiratory tract infection may yield a clinically relevant prolongation in time to extubation.
Keywords: CHD, congenital heart disease; ICU, intensive care unit; NPA, nasopharyngeal aspirate; PCICU, pediatric cardiac intensive care unit; RSV, respiratory syncytial virus; RTI, respiratory tract infection; VIS, vasoactive inotropic score; WCCHN, Western Canadian Congenital Heart Network; congenital heart disease; intensive care units; pediatrics; postoperative outcomes; viral respiratory tract infections.
© 2021 The Author(s).
Figures
References
-
- Meissner C.H. Viral bronchiolitis in children. N Engl J Med. 2016;374:62–72. - PubMed
-
- MacDonald N.E., Hall C.B., Suffin S.C., Alexon C., Harris P.J., Manning J.A. Respiratory syncytial viral infection in infants with congenital heart disease. N Engl J Med. 1982;307:397–400. - PubMed
-
- Feldman R.J., Fidalgo H.C., John J.F., Jr. Respiratory syncytial virus infection in a cardiac surgery intensive care unit. J Thorac Cardiovasc Surg. 1994;108:1152. - PubMed
-
- Malviya S., Voepel-Lewis T., Siewert M., Pandit U.A., Riegger L.Q., Tait A.R. Risk factors for adverse postoperative outcomes in children presenting for cardiac surgery with upper respiratory tract infections. Anesthesiology. 2003;98:628–632. - PubMed
-
- Delgado-Corcoran C., Witte M.K., Ampofo K., Castillo R., Bodily S., Bratton S.L. The impact of human rhinovirus infection in pediatric patients undergoing heart surgery. Pediatr Cardiol. 2014;35:1387–1394. - PubMed
LinkOut - more resources
Full Text Sources
