

Permanent pacemaker placement following valve surgery is not independently associated with worse outcomes
- PMID: 36003744
- PMCID: PMC9390660
- DOI: 10.1016/j.xjon.2021.06.005
Permanent pacemaker placement following valve surgery is not independently associated with worse outcomes
Abstract
Background: Permanent pacemaker placement (PPM) is associated with morbidity following cardiac surgery. This study identified associations between PPM placement and 5-year outcomes for patients that require PPM following valvular surgery.
Methods: All patients who underwent valvular surgery at our medical center from 2011 to 2018 were considered for analysis. Multivariable analysis identified associations between PPM placement, mortality, and readmissions. Primary outcomes were operative complications and mortality. Secondary outcomes included 5-year survival and readmission.
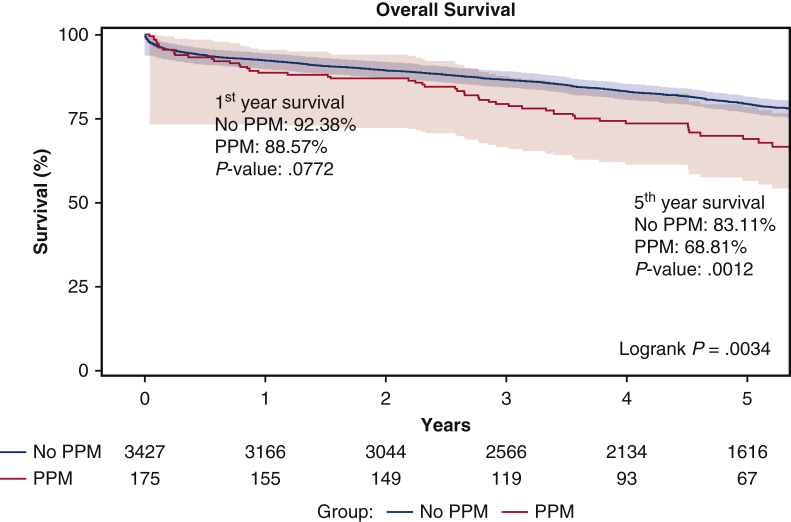
Results: A total of 175 (4.86%) of 3602 valvular surgery patients required postoperative PPM. The PPM cohort had significantly worse baseline comorbidities, including greater Society of Thoracic Surgeons Predicted Risk of Mortality (STS-PROM) scores (3.8 vs 2.4 P < .0001). The PPM cohort had greater rates of blood product transfusion, prolonged ventilation, and new-onset atrial fibrillation. PPM placement was significantly associated with third-degree heart block (5.26; 95% confidence interval [95% CI], 1.00-27.53; P = .0496), ventricular fibrillation/tachycardia (3.90; 95% CI, 1.59-9.59; P = .01), and atrial fibrillation/flutter (1.53; 95% CI, 1.05-2.24; P = .03). On Kaplan-Meier estimates, 5-year survival (68.8% vs 83.1%; P = 01) was significantly reduced in the PPM cohort. Five-year all-cause readmission (60.4% vs 50.04%; P = .01) and heart failure readmission (35.5% vs 20.1%; P < .000) occurred more frequently in the PPM cohort. On multivariable Cox regression analysis, PPM placement (hazard ratio, 1.12; 95% CI, 0.84-1.50; P = .444) was not an independent predictor of mortality. On competing risk analysis, PPM (hazard ratio, 1.33; 95% CI, 0.99-1.80; P = .062) was not a predictor of hospital readmission.
Conclusions: Valvular surgery patients who required postoperative PPM had elevated baseline operative risk. However, PPM implantation was not associated with mortality or readmission.
Keywords: CABG, coronary artery bypass grafting; CI, confidence interval; HR, hazard ratio; ICD, implantable cardioverter-defibrillator; PPM, postoperative pacemaker placement; arrythmia; permanent pacemaker (PPM); valve surgery.
© 2021 The Authors.
Figures







Similar articles
-
Pacemaker Implantation After Mitral Valve Surgery With Atrial Fibrillation Ablation.J Am Coll Cardiol. 2019 May 21;73(19):2427-2435. doi: 10.1016/j.jacc.2019.02.062. J Am Coll Cardiol. 2019. PMID: 31097163 Free PMC article. Clinical Trial.
-
Need for Permanent Pacemaker After Surgical Aortic Valve Replacement Reduces Long-Term Survival.Ann Thorac Surg. 2018 Aug;106(2):460-465. doi: 10.1016/j.athoracsur.2018.02.041. Epub 2018 Mar 22. Ann Thorac Surg. 2018. PMID: 29577930 Free PMC article.
-
Incidence, Predictors, and Outcomes of Permanent Pacemaker Implantation Following Transcatheter Aortic Valve Replacement: Analysis From the U.S. Society of Thoracic Surgeons/American College of Cardiology TVT Registry.JACC Cardiovasc Interv. 2016 Nov 14;9(21):2189-2199. doi: 10.1016/j.jcin.2016.07.026. JACC Cardiovasc Interv. 2016. PMID: 27832844
-
Tricuspid regurgitation associated with implantable electrical device insertion: A systematic review and meta-analysis.Pacing Clin Electrophysiol. 2021 Aug;44(8):1297-1302. doi: 10.1111/pace.14287. Epub 2021 Jul 1. Pacing Clin Electrophysiol. 2021. PMID: 34081789
-
Endovascular stent grafting and open surgical replacement for chronic thoracic aortic aneurysms: a systematic review and prospective cohort study.Health Technol Assess. 2022 Jan;26(6):1-166. doi: 10.3310/ABUT7744. Health Technol Assess. 2022. PMID: 35094747
Cited by
-
Predictors of Survival After Triple Valve Surgery: A Single Center Analysis.Ann Thorac Surg Short Rep. 2024 Aug 8;3(1):25-30. doi: 10.1016/j.atssr.2024.07.021. eCollection 2025 Mar. Ann Thorac Surg Short Rep. 2024. PMID: 40098837 Free PMC article.
-
Commentary: If you start me up…I may never stop?JTCVS Open. 2021 Jul 22;7:165-166. doi: 10.1016/j.xjon.2021.07.020. eCollection 2021 Sep. JTCVS Open. 2021. PMID: 36003722 Free PMC article. No abstract available.
-
Commentary: Permanent pacemaker implantation after cardiac surgery: Are we getting distracted by the usual suspects?JTCVS Open. 2021 Jul 2;7:167-168. doi: 10.1016/j.xjon.2021.06.025. eCollection 2021 Sep. JTCVS Open. 2021. PMID: 36003699 Free PMC article. No abstract available.
References
-
- Bis J., Gościńska-Bis K., Gołba K.S., Gocoł R., Zębalski M., Deja M.A. Permanent pacemaker implantation after cardiac surgery: optimization of the decision making process. J Thorac Cardiovasc Surg. February 19, 2020 [Epub ahead of print] - PubMed
-
- Del Rizzo D.F., Nishimura S., Lau C., Sever J., Goldman B.S. Cardiac pacing following surgery for acquired heart disease. J Card Surg. 1996;11:332–340. - PubMed
-
- Gordon R.S., Ivanov J., Cohen G., Ralph-Edwards A.L. Permanent cardiac pacing after a cardiac operation: predicting the use of permanent pacemakers. Ann Thorac Surg. 1998;66:1698–1704. - PubMed
LinkOut - more resources
Full Text Sources
