

Hypertension is prevalent in non-alcoholic fatty liver disease and increases all-cause and cardiovascular mortality
- PMID: 36003916
- PMCID: PMC9393330
- DOI: 10.3389/fcvm.2022.942753
Hypertension is prevalent in non-alcoholic fatty liver disease and increases all-cause and cardiovascular mortality
Abstract
Background and aims: Hypertension (HTN) is a common comorbidity in non-alcoholic fatty liver disease (NAFLD) affecting up to 40% of individuals. However, the impact of HTN and its control on outcomes in NAFLD remains unclear. Therefore, we aimed to examine the impact of HTN on survival outcomes in a longitudinal cohort of NAFLD patients.
Methods: The analysis consisted of adults in the National Health and Nutrition Examination Survey (NHANES) from 1999 to 2018 with data on socio-demographic characteristics and comorbidities. NAFLD was diagnosed with fatty liver index (FLI) and United States-FLI at a cut-off of 60 and 30, respectively in the substantial absence of alcohol use. A multivariate regression analysis was conducted to adjust for confounders.
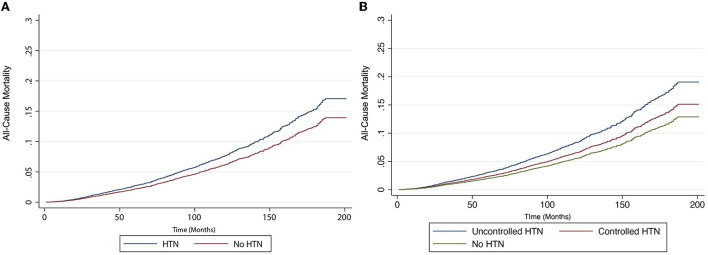
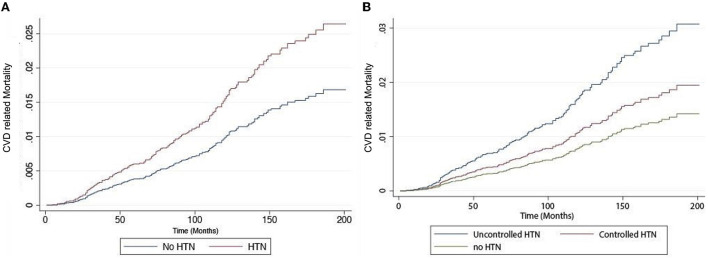
Results: A total of 45,302 adults were included, and 27.83% were identified to have NAFLD. Overall, 45.65 and 35.12% of patients with NAFLD had HTN and uncontrolled HTN, respectively. A multivariate analysis with confounders demonstrated that hypertensive NAFLD had a significantly increased risk of all-cause mortality (HR: 1.39, CI: 1.14-1.68, p < 0.01) and cardiovascular disease (CVD) mortality (HR: 1.85, CI: 1.06-3.21, p = 0.03). Untreated HTN remained to have a significantly increased risk in all-cause (HR: 1.59, CI: 1.28-1.96, p < 0.01) and CVD mortality (HR: 2.36, CI: 1.36-4.10, p < 0.01) while treated HTN had a non-significant increased risk of CVD mortality (HR: 1.51, CI: 0.87-2.63, p = 0.14) and a lower magnitude of increase in the risk of all-cause mortality (HR: 1.26, CI: 1.03-1.55, p = 0.03).
Conclusion: Despite the significant burden of HTN in NAFLD, up to a fifth of patients have adequate control, and the lack thereof significantly increases the mortality risk. With the significant association of HTN in NAFLD, patients with NAFLD should be managed with a multidisciplinary team to improve longitudinal outcomes.
Keywords: cardiovascular; controlled hypertension; mortality; non-alcoholic fatty liver (NAFL); uncontrolled hypertension.
Copyright © 2022 Ng, Wong, Chew, Chan, Xiao, Sayed, Lim, Tan, Loke, Tay, Yong, Kong, Huang, Wang, Chan, Dalakoti, Tamaki, Noureddin, Siddiqui, Sanyal and Muthiah.
Conflict of interest statement
Author AS is President of Sanyal Biotechnology and has stock options in Genfit, Akarna, Tiziana, Indalo, Durect, and Galmed. He has served as a consultant to Astra Zeneca, Nitto Denko, Enyo, Ardelyx, Conatus, Nimbus, Amarin, Salix, Tobira, Takeda, Jannsen, Gilead, Terns, Birdrock, Merck, Valeant, Boehringer-Ingelheim, Lilly, Hemoshear, Zafgen, Novartis, Novo Nordisk, Pfizer, Exhalenz, and Genfit. He has been an unpaid consultant to Intercept, Echosens, Immuron, Galectin, Fractyl, Syntlogic, Affimune, Chemomab, Zydus, Nordic Bioscience, Albireo, Prosciento, Surrozen, and Bristol Myers Squibb. His institution has received grant support from Gilead, Salix, Tobira, Bristol Myers, Shire, Intercept, Merck, Astra Zeneca, Malinckrodt, Cumberland, and Norvatis. He receives royalties from Elsevier and UptoDate. Author MN has been on the advisory board for 89BIO, Gilead, Intercept, Pfizer, Novo Nordisk, Blade, EchoSens, Fractyl, Terns, Siemens, and Roche diagnostic; He has received research support from Allergan, BMS, Gilead, Galmed, Galectin, Genfit, Conatus, Enanta, Madrigal, Novartis, Pfizer, Shire, Viking, and Zydus. He is a minor shareholder or has stocks in Anaetos, Rivus Pharma, and Viking. Author MC has received speaker's fees and research grants Astra Zeneca, Abbott Technologies, and Boston Scientific. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources