

Stentless valves for bicuspid and tricuspid aortic valve disease
- PMID: 36004130
- PMCID: PMC9390591
- DOI: 10.1016/j.xjon.2021.09.033
Stentless valves for bicuspid and tricuspid aortic valve disease
Abstract
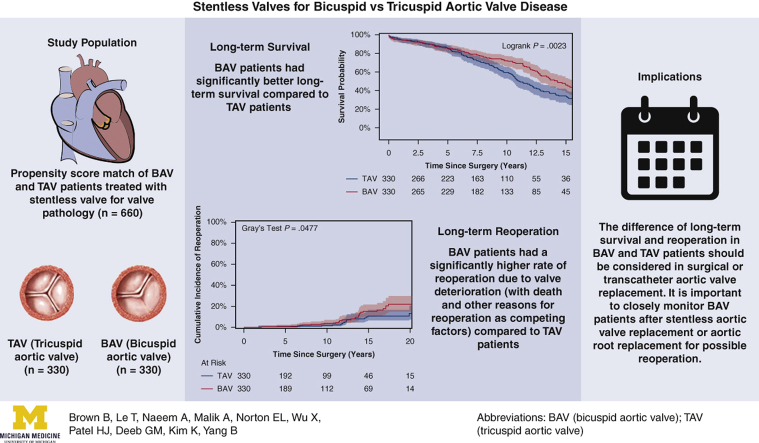
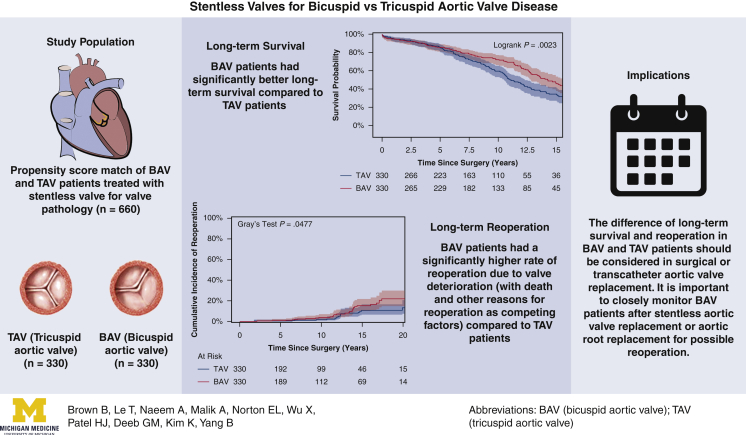
Objective: To determine long-term survival and reoperation rate in patients with a bicuspid aortic valve (BAV) and patients with a tricuspid aortic valve (TAV) after stentless aortic valve replacement (AVR)/aortic root replacement (ARR).
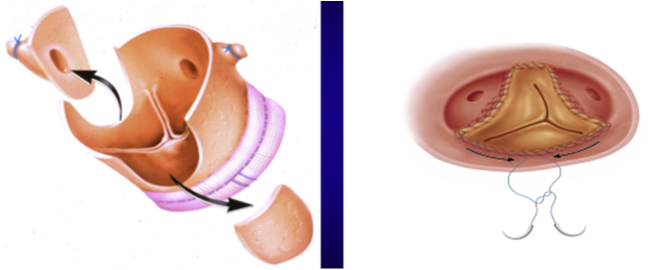
Methods: Between 1992 and 2014, 1293 patients underwent first AVR/ARR with a stentless aortic valve using the modified inclusion operating technique, including 741 patients with a TAV and 552 with a BAV. Using propensity scoring with 26 variables, 330 matched pairs were identified with AVR with or without ascending aorta/arch replacement. Data were obtained through chart review, surveys, and the National Death Index.
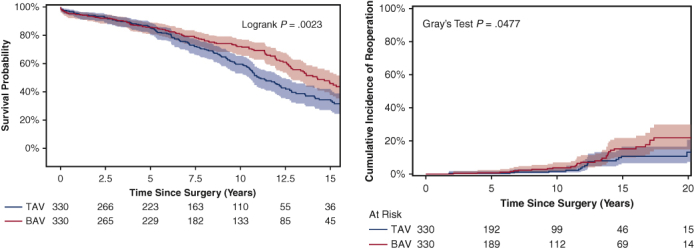
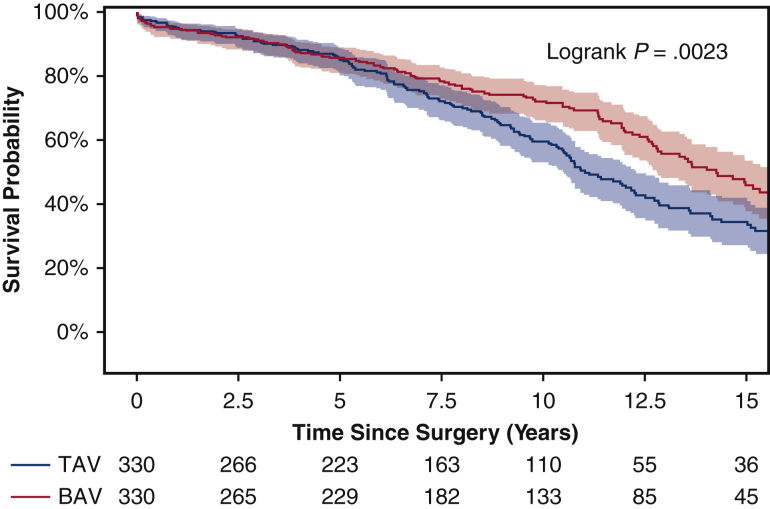
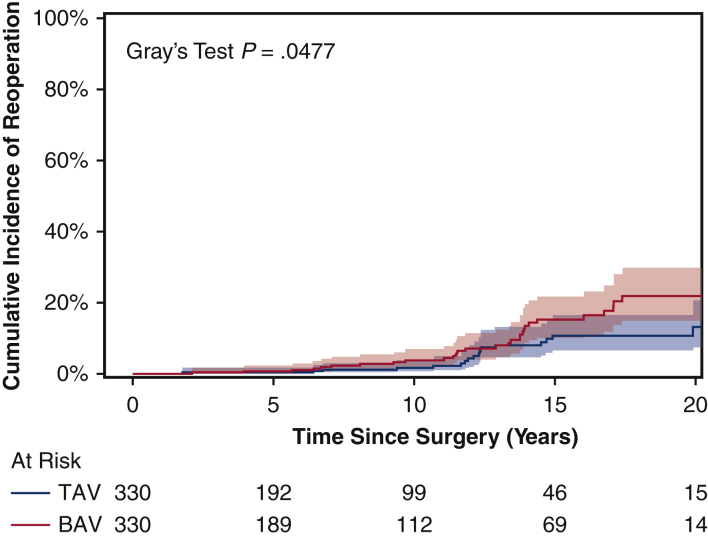
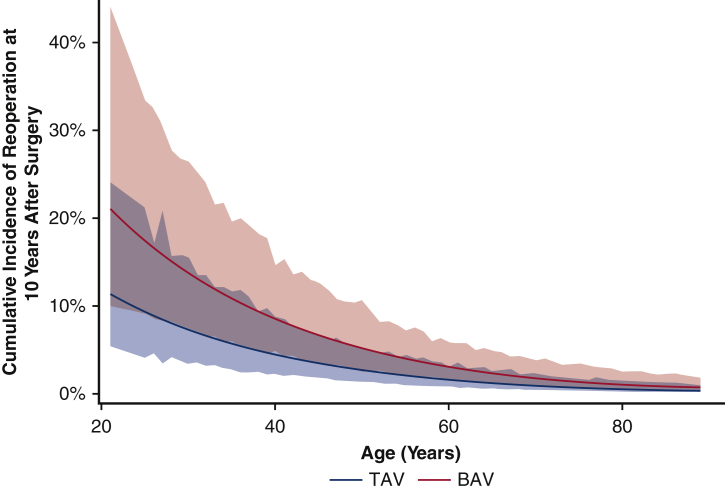
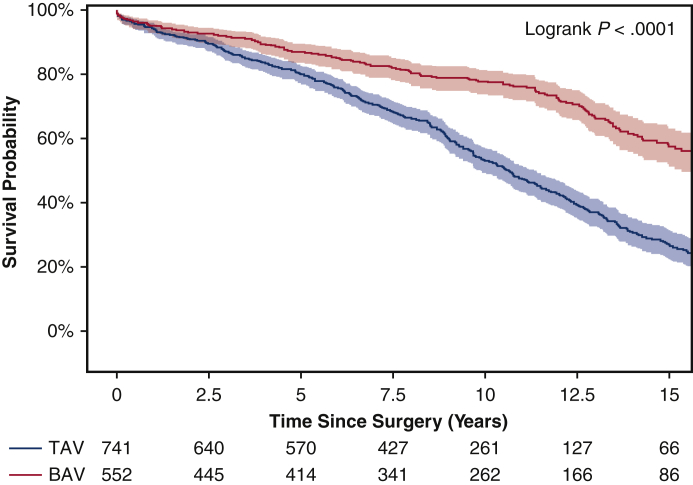
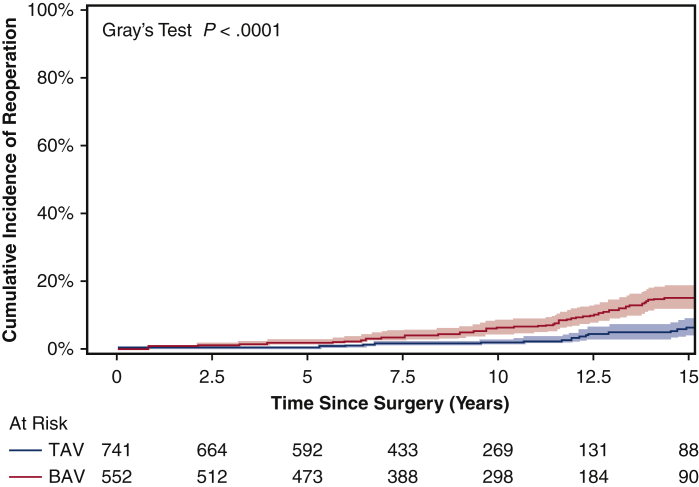
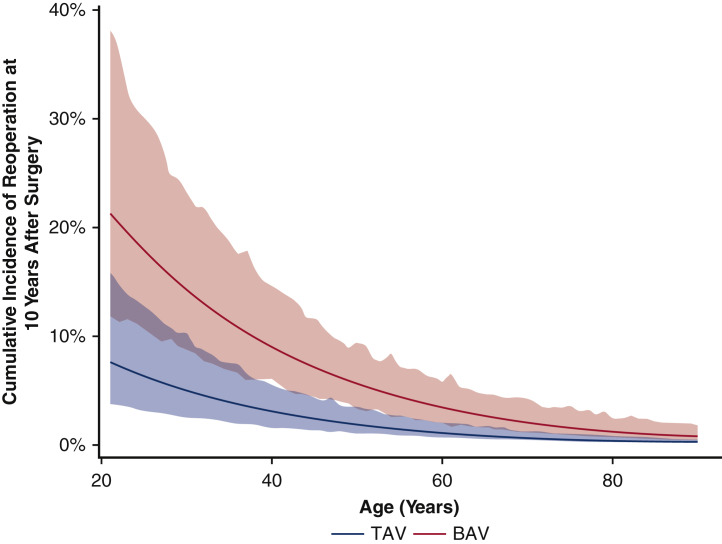
Results: Patient demographics were similar in the propensity score-matched groups. Both groups had similar cardiopulmonary bypass, cross-clamp, and hypothermia circulatory arrest times, cerebral protection strategies, and rate of aortic arch replacement. The median size of implanted valves was similar (BAV: 27 mm [range, 25-29 mm] vs TAV: 27 mm [range, 25-27 mm]). Compared with the TAV group, the BAV group had a shorter hospital stay (6 days vs 7 days; P = .001) but similar 30-day mortality (1.8% vs 1.2%). The BAV group had better long-term (15-year) survival (46% vs 33%; P = .002) but a higher cumulative incidence of reoperation for structural valve deterioration (15-year: 15% vs 11%; P = .048). Cox proportional hazard analysis identified a BAV as a protective factor for long-term mortality (hazard ratio [HR], 0.71; 95% CI, 0.56-0.91; P = .006), but a risk factor for reoperation due to structural valve deterioration (HR, 1.4 [95% CI, 0.8-2.6; P = .27] in the matched cohort and 2.2 [95% CI, 1.3-3.7; P = .004] in the unmatched cohort).
Conclusions: The BAV patients had better long-term survival but a higher reoperation rate compared with TAV patients after stentless AVR. Our findings suggest caution in the use of bioprostheses for BAV patients.
Keywords: AVR, aortic valve replacement; BAV, bicuspid aortic valve; CI, confidence interval; HR, hazard ratio; NDI, National Death Index; OR, odds ratio; SAVR, surgical aortic valve replacement; TAV, tricuspid aortic valve; TAVR, transcatheter aortic valve replacement; aortic valve replacement; bicuspid aortic valve; bioprosthesis; long-term survival; reoperation; stentless valve.
© 2021 The Author(s).
Figures
References
-
- Centers for Disease Control and Prevention National Center for Health Statistics. National death index. https://www.cdc.gov/nchs/ndi/index.htm Available at:
-
- Clark T.G., Altman D.G., De Stavola B.L. Quantification of the completeness of follow-up. Lancet. 2002;359:1309–1310. - PubMed
-
- Ali A., Patel A., Ali Z.A., Abu-Omar Y., Freed D., Sheikh A.Y., et al. Stentless aortic valve replacement in patients with bicuspid aortic valve disease: clinical outcome and aortic diameter changes during follow-up. Eur J Cardiothorac Surg. 2010;38:134–140. - PubMed
-
- Haunschild J., Misfeld M., Schroeter T., Lindemann F., Davierwala P., von Aspern K., et al. Prevalence of permanent pacemaker implantation after conventional aortic valve replacement—a propensity-matched analysis in patients with a bicuspid or tricuspid aortic valve: a benchmark for transcatheter aortic valve replacement. Eur J Cardiothorac Surg. 2020;58:130–137. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
